
This study aims to evaluate the involvement of hospital pharmacists in the protocolization, management and clinical follow-up of non-cytotoxic drug extravasations in Spanish hospitals.
MethodsA survey was distributed through the SEFH email list using the REDCap® web platform. The characteristics of the participating hospitals, the availability of a protocol for managing non-cytotoxic drug extravasations, the healthcare professionals involved in developing the protocol, and the pharmacists' involvement and clinical follow-up in response to these incidents were investigated.
ResultsA total of 89 complete responses were obtained from hospitals across 14 Autonomous Communities. Only 12 centers (13.5%) had a protocol that included recommendations for the extravasation of non-cytotoxic drugs, and in 11 (91.7%) of these, the pharmacist had participated in its development. The recommendations for extravasation management were mainly based on intrinsic drug properties such as pH and osmolarity, specific properties like vasoconstrictor drugs, or the classification of drugs as vesicants, irritants, or non-irritants. Wide variability was observed in recommendations regarding the application of cold or heat and hyaluronidase dosage. The decision to consult with pharmacy service regarding the management of extravasation depended largely on the individual nurse or physician's judgment, but 20 centers (22.5%) reported that they never received such consultations. A large proportion of Pharmacy Services (73.0%) reported that they participate in extravasation management by providing information by telephone, but 21 centers (23.6%) indicated that the pharmacist never participates in these adverse events. Limited involvement was also noted in the clinical assessment of the patient, follow-up of the extravasation, and documentation in the patient's medical history.
ConclusionThe results of this survey reflect the limited standardization in the management of non-cytotoxic drug extravasations, as well as significant heterogeneity in the level of involvement of hospital pharmacists in these adverse events across hospitals in our country. The need to establish a national guideline or document on the management of non-cytotoxic drug extravasations is highlighted, along with the importance of promoting interdisciplinary collaboration to improve patient safety.
conocer el grado de implicación de los farmacéuticos hospitalarios en la protocolización, el manejo y el seguimiento clínico de las extravasaciones de medicamentos no citotóxicos en los hospitales españoles.
Métodosse realizó una encuesta en la plataforma web REDCap®, que se difundió a través de la lista de distribución de correo de la Sociedad Española de Farmacia Hospitalaria. Se consultaron las características de los hospitales participantes, la protocolización del manejo de las extravasaciones de fármacos no citotóxicos y los profesionales sanitarios que participaron en la elaboración del protocolo, así como la implicación y el seguimiento clínico de los farmacéuticos ante estos incidentes.
Resultadosse obtuvieron 89 respuestas completas del cuestionario, procedentes de hospitales de 14 comunidades autónomas. Únicamente 12 centros (13,5%) disponían de un protocolo que incluía recomendaciones para las extravasaciones de medicamentos no citotóxicos, y en 11 (91,7%) de ellos el farmacéutico había participado en su elaboración. Las recomendaciones se basaban principalmente en propiedades intrínsecas a los fármacos, como el pH y la osmolaridad, en propiedades específicas como la vasoconstricción, o en su clasificación como vesicantes, irritantes o no irritantes. Se observó una gran variabilidad en las recomendaciones de cuándo aplicar frío o calor, o en la dosificación de hialuronidasa. Las consultas a los servicios de farmacia sobre el manejo de las extravasaciones dependían principalmente del criterio individual del enfermero o del médico, y en 20 centros (22,5%) se reportó que nunca recibían este tipo de consultas. Una gran parte de los servicios de farmacia (73,0%) reportó que participa en el manejo de la extravasación, proporcionando información por vía telefónica, pero en 21 centros (23,6%) se indicó que el farmacéutico nunca participa en estos acontecimientos adversos. Se observó también una escasa participación en la valoración clínica del paciente, el seguimiento de la extravasación y su registro en la historia clínica del paciente.
Conclusiónlos resultados de la encuesta reflejan la escasa protocolización del manejo de las extravasaciones por fármacos no citotóxicos, así como una notable heterogeneidad en el grado de implicación del farmacéutico hospitalario en estos eventos adversos en los hospitales de nuestro país. Se destaca la necesidad de establecer una guía o documento nacional sobre el manejo de las extravasaciones de medicamentos no citotóxicos, así como de fomentar la colaboración interdisciplinaria para mejorar la seguridad del paciente.
The intravenous administration of medications can result in the unintentional leakage of fluid into perivascular or subcutaneous spaces.1 Although these incidents may have minimal consequences, they can sometimes lead to serious injuries with long-term sequelae, particularly in the case of vesicant medications.
The terms extravasation and infiltration are often used interchangeably in the literature. However, the 2024 Infusion Therapy Practice Standards2 define extravasation as the “unintended infiltration of a vesicant solution or medication into surrounding tissue”, whereas infiltration refers to the “unintended administration of a non-vesicant solution or medication into surrounding tissues.”
The scientific literature suggests that the incidence rate of extravasation in the general population ranges from 0.1% to 0.7%.3 When analysed by therapeutic group, cytotoxic agents have the highest incidence rate, ranging from 0.1% to 6%. The reported incidence rate is even higher in the paediatric and neonatal population, ranging from 11% to 58%. These rates may be significantly underestimated due to the absence of a centralised incident registry.4
The impact of extravasation is mainly determined by its location and volume, although the physicochemical properties of the drugs also play a crucial role.5
Although there are specific recommendations for managing specific drugs or therapeutic groups, such as radiological contrast media6 or antineoplastic agents,7 information on other drugs is limited or absent. Such information is derived only from the isolated experience of certain authors or hospitals and is not supported by larger studies. In exceptional cases, indications for their management can only be found in the Summary of Product Characteristics for medicines.
Due to their knowledge of the physicochemical properties of medicines (e.g., pH, osmolarity), pharmacists can provide guidance on managing extravasation and assessing the potential risks of these incidents. Their involvement is essential for optimising the management of an extravasation event using a multidisciplinary approach that includes patients, nurses, pharmacists, and doctors. Furthermore, implementing standardised protocols for managing cytotoxic and non-cytotoxic drug extravasations in healthcare institutions can help to improve prevention and reduce associated complications.5
The aim of this study was to determine the extent to which hospital pharmacists are involved in the protocolisation, management, and clinical follow-up of non-cytotoxic drug extravasations in Spanish hospitals. This was done in order to subsequently assess the need to develop a protocol or consensus document to guide pharmacists and other healthcare professionals in managing these incidents.
MethodsAn online survey on non-cytotoxic drug extravasation was designed by the Clinical Safety Working Group of the Spanish Society of Hospital Pharmacy (SEFH) using the REDCap-SEFH web platform. The survey was approved by all group members. As no clinical data were to be collected, the study did not require approval from the drug research ethics committees. In addition, the information provided by the hospitals was aggregated and anonymised.
The survey was distributed via the SEFH members' email distribution list in February 2024 and was available for a period of 30 days. Only 1 response per hospital was allowed.
The questionnaire was divided into 3 sections (see Appendix). The first section collected information on the characteristics of each hospital including its autonomous community, type of hospital (Groups 1 to 6, according to the “Classification of Spanish public hospitals using cluster analysis”),8 funding model, number of beds, healthcare coverage, and specific clinical services offered. The number of specialist pharmacists and the availability of accreditation for specialised healthcare training were also documented. The second section collected information on the availability of an internal protocol for managing non-cytotoxic drug extravasations or any related protocol, the participation of pharmacists in its development, the drug properties on which the protocol recommendations are based, and the pharmacological and non-pharmacological recommendations themselves.
The third section addressed the notification of such adverse events to the pharmacy service, the pharmacy service's involvement in these consultations, the type of recommendations made (e.g., general or specific), how this activity is documented, and the availability of antidotes for extravasations. In addition, the respondents were asked if they thought a protocol or guideline for managing these extravasations was needed.
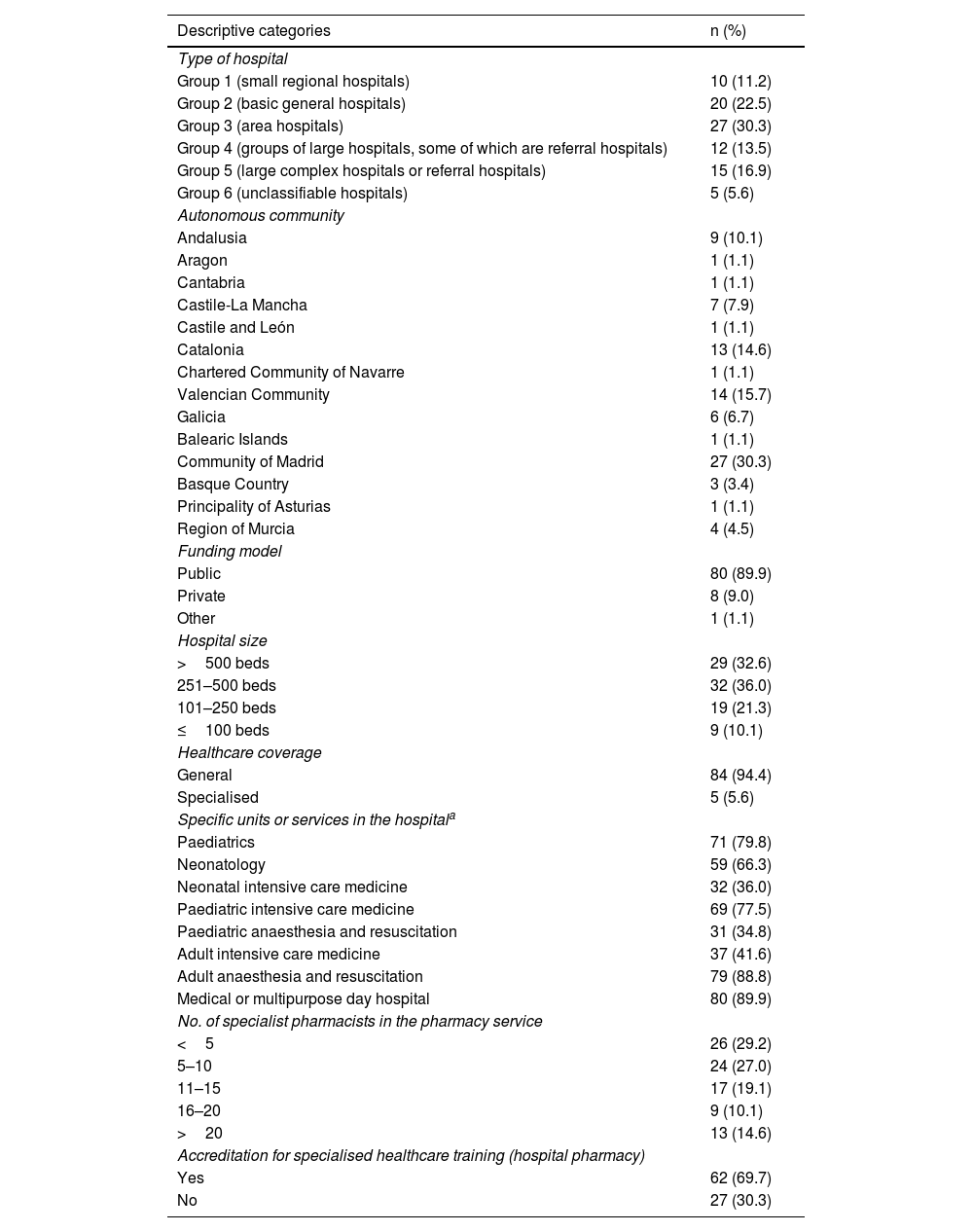
ResultsA total of 90 responses were obtained. One response was discarded as it was incomplete. Hospitals across 14 autonomous communities participated. Table 1 shows the geographical distribution of the participating hospitals and their characteristics.
Characteristics of participating hospitals and corresponding pharmacy services.
| Descriptive categories | n (%) |
|---|---|
| Type of hospital | |
| Group 1 (small regional hospitals) | 10 (11.2) |
| Group 2 (basic general hospitals) | 20 (22.5) |
| Group 3 (area hospitals) | 27 (30.3) |
| Group 4 (groups of large hospitals, some of which are referral hospitals) | 12 (13.5) |
| Group 5 (large complex hospitals or referral hospitals) | 15 (16.9) |
| Group 6 (unclassifiable hospitals) | 5 (5.6) |
| Autonomous community | |
| Andalusia | 9 (10.1) |
| Aragon | 1 (1.1) |
| Cantabria | 1 (1.1) |
| Castile-La Mancha | 7 (7.9) |
| Castile and León | 1 (1.1) |
| Catalonia | 13 (14.6) |
| Chartered Community of Navarre | 1 (1.1) |
| Valencian Community | 14 (15.7) |
| Galicia | 6 (6.7) |
| Balearic Islands | 1 (1.1) |
| Community of Madrid | 27 (30.3) |
| Basque Country | 3 (3.4) |
| Principality of Asturias | 1 (1.1) |
| Region of Murcia | 4 (4.5) |
| Funding model | |
| Public | 80 (89.9) |
| Private | 8 (9.0) |
| Other | 1 (1.1) |
| Hospital size | |
| >500 beds | 29 (32.6) |
| 251–500 beds | 32 (36.0) |
| 101–250 beds | 19 (21.3) |
| ≤100 beds | 9 (10.1) |
| Healthcare coverage | |
| General | 84 (94.4) |
| Specialised | 5 (5.6) |
| Specific units or services in the hospitala | |
| Paediatrics | 71 (79.8) |
| Neonatology | 59 (66.3) |
| Neonatal intensive care medicine | 32 (36.0) |
| Paediatric intensive care medicine | 69 (77.5) |
| Paediatric anaesthesia and resuscitation | 31 (34.8) |
| Adult intensive care medicine | 37 (41.6) |
| Adult anaesthesia and resuscitation | 79 (88.8) |
| Medical or multipurpose day hospital | 80 (89.9) |
| No. of specialist pharmacists in the pharmacy service | |
| <5 | 26 (29.2) |
| 5–10 | 24 (27.0) |
| 11–15 | 17 (19.1) |
| 16–20 | 9 (10.1) |
| >20 | 13 (14.6) |
| Accreditation for specialised healthcare training (hospital pharmacy) | |
| Yes | 62 (69.7) |
| No | 27 (30.3) |
Total sample = 89.
Only 12 hospitals (13.5%) had a protocol that included recommendations for non-cytotoxic drug extravasation. Pharmacists had participated in developing the protocol in 11 of these hospitals (91.7%), nurses and doctors were involved in 6 hospitals (50.0%), and surgeons participated in 2 of these 6 hospitals.
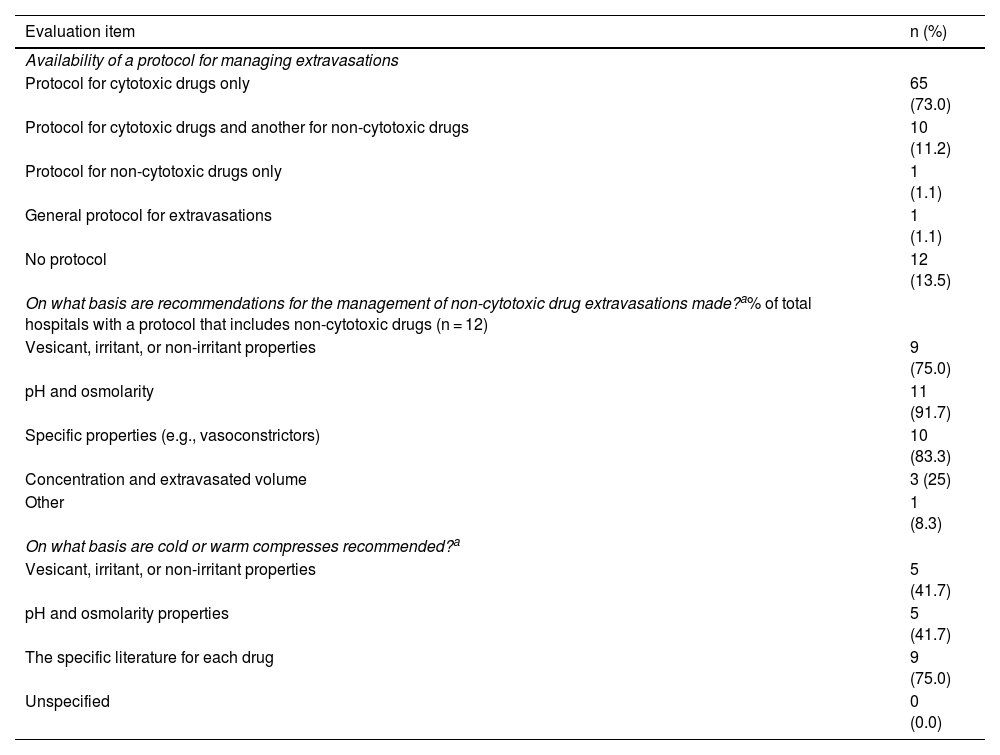
Table 2 shows the type of protocols available in the participating hospitals and the recommendations for managing extravasations. The recommended guidelines for the use of cold or warm compresses were specified by only 7 hospitals, and there were marked variations in the duration and number of daily applications. The most common guideline (n = 5) for the use of cold compresses was 20 min (range 15–60 min), 4 times a day (range 3–6), for 2 days (range 1–3), whereas for warm compresses (n = 4), it was 20 min (range 15–20 min), 4 times a day (range 3–4), for 2 days (range 1–3).
Type of protocols available and recommendations for managing non-cytotoxic drug extravasations.
| Evaluation item | n (%) |
|---|---|
| Availability of a protocol for managing extravasations | |
| Protocol for cytotoxic drugs only | 65 (73.0) |
| Protocol for cytotoxic drugs and another for non-cytotoxic drugs | 10 (11.2) |
| Protocol for non-cytotoxic drugs only | 1 (1.1) |
| General protocol for extravasations | 1 (1.1) |
| No protocol | 12 (13.5) |
| On what basis are recommendations for the management of non-cytotoxic drug extravasations made?a% of total hospitals with a protocol that includes non-cytotoxic drugs (n = 12) | |
| Vesicant, irritant, or non-irritant properties | 9 (75.0) |
| pH and osmolarity | 11 (91.7) |
| Specific properties (e.g., vasoconstrictors) | 10 (83.3) |
| Concentration and extravasated volume | 3 (25) |
| Other | 1 (8.3) |
| On what basis are cold or warm compresses recommended?a | |
| Vesicant, irritant, or non-irritant properties | 5 (41.7) |
| pH and osmolarity properties | 5 (41.7) |
| The specific literature for each drug | 9 (75.0) |
| Unspecified | 0 (0.0) |
Total sample = 89.
The most common regimen (n = 8) for hyaluronidase involved subcutaneous injection of 150 IU, administered as 4 to 6 injections of 0.2 mL from the 150 IU/mL formulation. However, the reconstitution volume of the lyophilised hyaluronidase powder, and therefore the final concentration of the vial, varied considerably. This resulted in a wide dosage range (12–1800 IU) and variable numbers and volumes of administrations. Only 1 hospital (1.1%) included Burow's solution (aluminium acetate) in its recommendations.
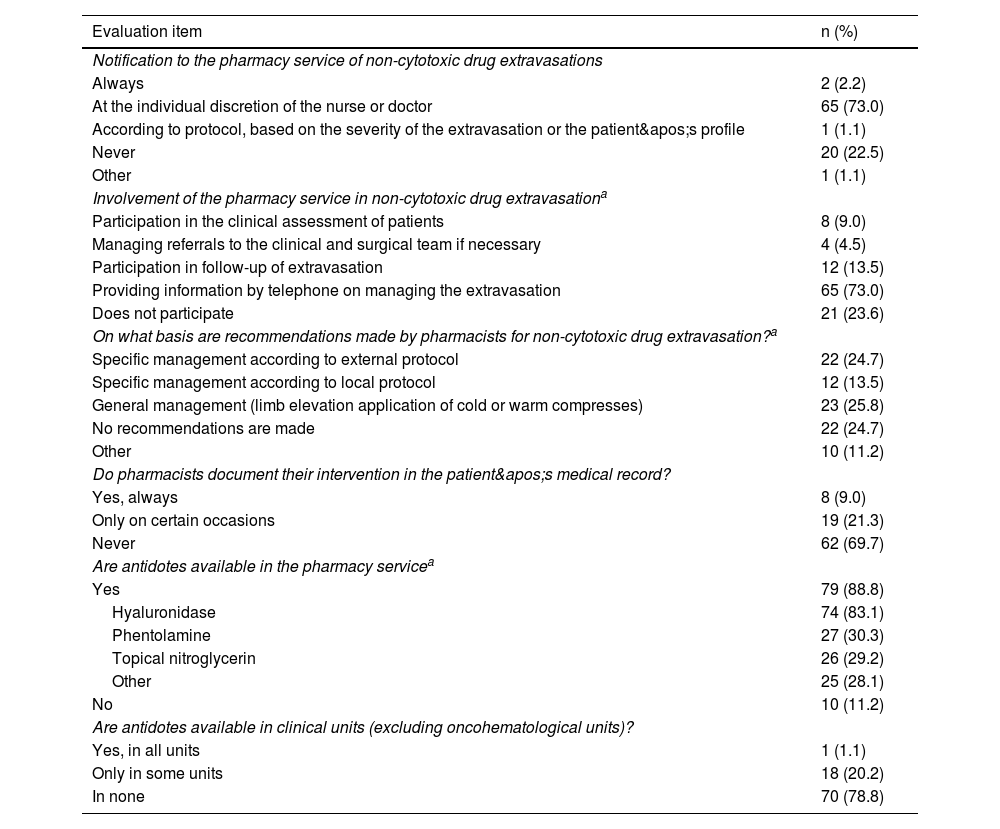
Table 3 shows the results relating to the reporting of extravasations by pharmacy services, the involvement of pharmacists in these consultations, the types of recommendations made, how often this activity was documented, and the availability of antidotes for extravasations.
Participation of the pharmacy service in non-cytotoxic drug extravasations, source of recommendations, and availability of antidotes.
| Evaluation item | n (%) |
|---|---|
| Notification to the pharmacy service of non-cytotoxic drug extravasations | |
| Always | 2 (2.2) |
| At the individual discretion of the nurse or doctor | 65 (73.0) |
| According to protocol, based on the severity of the extravasation or the patient's profile | 1 (1.1) |
| Never | 20 (22.5) |
| Other | 1 (1.1) |
| Involvement of the pharmacy service in non-cytotoxic drug extravasationa | |
| Participation in the clinical assessment of patients | 8 (9.0) |
| Managing referrals to the clinical and surgical team if necessary | 4 (4.5) |
| Participation in follow-up of extravasation | 12 (13.5) |
| Providing information by telephone on managing the extravasation | 65 (73.0) |
| Does not participate | 21 (23.6) |
| On what basis are recommendations made by pharmacists for non-cytotoxic drug extravasation?a | |
| Specific management according to external protocol | 22 (24.7) |
| Specific management according to local protocol | 12 (13.5) |
| General management (limb elevation application of cold or warm compresses) | 23 (25.8) |
| No recommendations are made | 22 (24.7) |
| Other | 10 (11.2) |
| Do pharmacists document their intervention in the patient's medical record? | |
| Yes, always | 8 (9.0) |
| Only on certain occasions | 19 (21.3) |
| Never | 62 (69.7) |
| Are antidotes available in the pharmacy servicea | |
| Yes | 79 (88.8) |
| Hyaluronidase | 74 (83.1) |
| Phentolamine | 27 (30.3) |
| Topical nitroglycerin | 26 (29.2) |
| Other | 25 (28.1) |
| No | 10 (11.2) |
| Are antidotes available in clinical units (excluding oncohematological units)? | |
| Yes, in all units | 1 (1.1) |
| Only in some units | 18 (20.2) |
| In none | 70 (78.8) |
Total sample = 89.
All respondents agreed on the need for a national guideline or consensus document on managing non-cytotoxic drug extravasations.
DiscussionA total of 89 hospitals participated in the survey, providing a moderately sized but diverse sample in terms of geographical distribution and level of healthcare complexity. The study included hospitals from almost all of Spain's autonomous communities, with the majority classified in complexity level group 3.
Few protocols were available on managing non-cytotoxic drug extravasations, with only 13.5% of hospitals having one. This result contrasts with those of the survey published in 2024 by the Spanish Oncology Pharmacy Group (GEDEFO) of the SEFH. It showed that a significantly higher percentage of Spanish hospitals (85.4%) reported having a protocol for managing cytotoxic drug extravasations.9 However, our study showed that pharmacists were involved in the development of protocols for non-cytotoxic drugs in almost all cases.
Most protocols base their recommendations for handling extravasation on physicochemical properties, such as pH and osmolarity, as well as on specific pharmacological properties, as in the case of vasoconstrictors. These criteria are consistent with the recommendations described in the scientific literature.1,7,10–13 However, it was observed that the concentration or volume of extravasated material is not usually considered when assessing the risk of injury, despite this factor being highlighted in multiple studies and guidelines.1,7,10,14–16 Neither is the severity of the extravasation systematically assessed.13,17
There was wide variability among the participating hospitals in terms of the properties taken into account when recommending the application of local cold or warm compresses. This result is consistent with the information in the available literature, which does not offer a standardised approach to locally treating non-cytotoxic drug extravasation. However, there is a consensus on the recommendation to apply local cold compresses in the event of extravasation of vesicant agents.10 In contrast, recommendations on the duration of each application and the number of treatment days are more diverse, possibly because this factor has not been studied in depth.
Regarding the recommendation for subcutaneous administration of hyaluronidase, there was also considerable variability in the reconstitution volume of the lyophilised vial, resulting in different concentrations of the reconstituted drug and, consequently, variations in the administered dose. The scientific literature recommends a range from 15 to 150 IU, reflecting the lack of consensus in this area.1,7,10 These differences in administered doses were also noted in the survey results on managing cytotoxic drugs, where the authors related them to the wide variability observed in the published literature. However, in Spain, it was clear that the standard practice relied on the use of intermediate doses, as recommended in the European Society for Medical Oncology/European Oncology Nursing Society clinical practice guidelines and by certain Spanish and European bodies.9,18 The recommendation to use Burow's water is anecdotal and coincides with the absence of this recommendation in the literature.
It was found that the involvement of pharmacists in managing extravasations was highly variable. Although some hospitals reported that pharmacists were actively involved in extravasations—participating in clinical assessments (9.0%), referrals to clinical teams or surgery (4.5%), and monitoring extravasations (13.5%)—the majority reported providing information by telephone (73.0%) or stated that they had not participated in these safety incidents (23.6%). While many pharmacy services are contacted solely at the discretion of the healthcare professional who detects the extravasation, over 20% of the participating hospitals stated that they never receive this type of consultation, suggesting a lack of awareness of the pharmacists' role in such events. In hospitals where consultations do take place, pharmacists stated that they mainly rely on external protocols or consult specific literature, due to the lack of internal protocols.
There are a few studies in the scientific literature that specifically describe the role of pharmacists in managing non-cytotoxic drug extravasation. As early as 1997, Mateu et al.11 highlighted the role of pharmacists in such incidents, considering their contribution valuable in searching the literature for useful information on managing extravasation, including clinical assessment, treatment, and patient follow-up. In 2020, Smoulders et al. emphasised the role of pharmacists in providing information on managing extravasation based on physicochemical properties, assessing potential risks, and actively participating in the development of institutional protocols. All of the above form part of a multidisciplinary approach involving patients, nurses, pharmacists, and doctors, with the aim of improving the extravasation treatment.5 Other authors have also highlighted the role of pharmacists in managing cytotoxic drug extravasation, highlighting the need for standardised management, updated recommendations based on available evidence, and monitoring and documenting the interventions carried out.19,20
Our survey showed that pharmacist interventions in non-cytotoxic drug extravasations are not routinely documented, with only 9% of hospitals documenting the consultations received. In contrast, this activity is significantly more standardised regarding cytotoxic drug extravasations. Jiménez-Pulido et al.9 found that 66.2% (45/68) of hospitals had a specific register for extravasations, although 22.2% (10/45) stated that it was not used in practice. There was a wide variation in the availability of antidotes between hospitals.
Although hyaluronidase was available in 88.8% (79) of pharmacy services, only 30% stocked phentolamine or topical nitroglycerin, both of which are necessary for managing extravasations of drugs with vasoconstrictive properties. In general, none were available in clinical units. This situation would be acceptable if antidotes could be dispensed without delay, 24 h a day, and if their administration were subject to a medical prescription and pharmaceutical validation. Having a protocol in place to prevent and manage extravasation and ensuring its proper distribution is key to improving patient safety.
A study conducted in Saudi Arabia found that only 9.6% of the 387 nursing professionals surveyed had adequate knowledge of how to manage non-cytotoxic drug extravasations.21 The authors suggested that protocolising extravasation management could significantly raise awareness of the potential harm of these events and reinforce the need for collaborative action to provide the best possible care.
This study has several limitations. Firstly, the results are based on a sample of hospitals that participated voluntarily and thus do not represent all hospitals in Spain. Secondly, although our survey enabled us to collect information on the various aspects under investigation, this methodological approach may overlook more nuanced aspects, and variations in the responses may not be reflected in the results.
In conclusion, the degree to which pharmacists are involved in managing non-cytotoxic drug extravasations varies considerably across hospitals in Spain. In most cases, pharmacists provide recommendations by telephone (73.0%) and some even participate in clinical assessment (9.0%) or patient follow-up (13.5%). However, 23.6% of hospitals acknowledged that their pharmacy service does not participate in managing this type of incident. The limited literature on this issue, coupled with the absence of agreed guidelines, means that the protocolisation of managing non-cytotoxic drug extravasation remains a challenge for many hospitals, as reflected in the survey results. It is clear that Spanish national guidelines or documentation on managing non-cytotoxic drug extravasations need to be established, and that interdisciplinary collaboration must be promoted to improve patient safety.
Contribution to the scientific literatureThis study highlights the absence of protocols for managing non-cytotoxic drug extravasations in hospitals in Spain, as well as significant differences in the degree of pharmacist involvement in the care and follow-up of patients involved in these incidents. The variability found in the recommended pharmacological and non-pharmacological measures reflects the lack of guidelines for managing many non-cytotoxic drugs.
In order to offer optimal management and promote interdisciplinary collaboration with the aim of improving patient safety, we emphasise the need for a Spanish national guideline or document compiling the best available evidence on non-cytotoxic drug extravasations.
Declaration of authorshipAll authors declare that they have made significant contributions to the manuscript. Each author participated in the following:
Inés Jiménez Lozano participated in conceiving the project, designing the survey, and data collection, analysis and interpretation. She was responsible for writing, reviewing, and preparing the article for submission.
Jose Manuel Caro Teller participated in conceiving the project, designing the survey, and data interpretation. He participated in writing and critically reviewing the article.
Montserrat Pérez Encinas, Helena Esteban Cartelle, Juan Manuel Rodríguez Camacho, María Jose Fernández Megía, Sergio Plata Paniagua, and María José Otero participated in designing the survey, interpreting the results, and critically reviewing the manuscript, making important intellectual contributions.
Inés Jiménez Lozano, María José Otero, and Montserrat Pérez Encinas approved the final version for publication.
None declared.

