


To present the requirements, development, structure and results of an electronic interconsultation platform (e-Interconsultation) for communication between primary and hospital care.
MethodA working group was created and set out its purposes, working schedule, software requirements, the structure of the electronic platform, validation procedure, and its implementation. Once the software had been developed and validated and training sessions were conducted, the electronic platform was launched in June 2015.
ResultsAfter 1 year of operation, a total of 321 electronic interconsultations had been made, 110 of which were referrals from hospital care to primary care in addition to 211 from primary to hospital care. The validation of prescriptions and the need for drug monitoring in primary care are among main reasons for consultation.
ConclusionsThe e-Interconsultation platform is a valid, efficient and user-friendly mean of consultation or patient referrals between both healthcare levels.
Presentar los requisitos, desarrollo, estructura y resultados de una plataforma de e-Interconsulta de comunicación entre farmacéuticos de atención primaria y hospitalaria.
MétodoSe creó un grupo de trabajo y se definieron los objetivos, el cronograma de trabajo, los requisitos del programa informático, la estructura de la plataforma electrónica, la validación de la misma y la implantación. Tras su desarrollo informático y su validación, se realizaron sesiones formativas y se puso en marcha en junio de 2015.
ResultadosTras un año de funcionamiento, el número total de e-interconsultas realizadas fue de 321, de las cuales 110 fueron derivaciones de atención hospitalaria hacia atención primaria y 211 en el sentido inverso. La homologación sanitaria de recetas y la necesidad de seguimiento farmacoterapéutico en atención primaria, destacan entre las causas motivadas de consulta.
ConclusionesLa plataforma e-Interconsulta, es un sistema válido, eficaz y de sencillo manejo para la derivación de consultas o pacientes entre ambos niveles asistenciales.
The e-Interconsultation platform discussed in this article is the first information system presented in Spain which comprises a mechanism collaborating in the process of patient transition from one of these care levels to the other, making it possible to standardize and document consultations, referrals and drug therapy care interventions.
This enables us to provide patients a higher quality and safety pharmaceutical care, to achieve more efficient and safer drug therapy monitoring, promoting co-responsibility of health outcomes and facilitates communications between professionals.
IntroductionHealthcare provided in Spanish National Health System has progressively evolved from a compartmentalized model into two large-scale structures, hospital care (HC) and primary care (PC), to a cross-sectional, horizontal, integrating model in which the patients are considered to be the center point regardless of the level of care in which they are located and who must be provided a continuous care1. This change in the care-providing model has also been incorporated and promoted in Spain’s different Regional Health Systems, especially over the last ten years, for the purpose of doing away with health care-related barriers and the management of chronic care2-6.
In keeping with this change in health care paradigm, hospital pharmaceutical care (HPC) has progressively turned into patient-oriented care and has begun fostering the seamlessness of this care, given that the transitions between different levels of care are a critical point in drug therapy quality and safety. In this regard, the reference professional scientific societies (SEFH -Spanish Society of Hospital Pharmacy- and ASPH-American Society of Healthsystem Pharmacists) are promoting initiatives and strategies promoting integral pharmaceutical care for patients (in-hospital, out-of-hospital and outpatient) via the incorporation of the new technologies for achieving the care-providing objective7-8.
Taking care continuity and the use of new technologies as the basis, in part, of chronic patient management, the mission of the Pharmacy Service at our hospital has been determined as “providing personalized pharmaceutical care for each patient, seeking the innovation and cooperation of the different care levels, based on transparency and having the goal to achieved results in our patients’ health”. Therefore, it is necessary for the hospital pharmacists and the primary care pharmacists to be in touch with one another in order to provide continuous pharmaceutical care. In our case, the reference hospital of the sanitary area is a top-level 1450-bed hospital covering the care of a health area totaling approximately 550,000 inhabitants, with 21 pharmacists on staff who are also responsible for the sociosanitary services (approx. 1,200 beds). Similarly, there are 12 PC pharmacists distributed among primary medical center (71) spread throughout the health area. Both levels (primary and hospital) are integrated under one same Integrated Management Administration (XXI), each one of which is under a separate medical management.
Communications between PC and HC pharmacists concerning specific patients in particular in our health area have been being carried out without any officially-approved procedure, normally by telephone or e-mail. However, as of two years ago, taking into account the aforementioned mission, the hospital’s Pharmacy Service and the XXIAC Primary Care Pharmacy Units have developed a two-way electronic (e-Interconsultation) platform between HC and PC pharmacists within this health area, with the support of Informatic Technology Service of the hospital, which has made it possible not only to carry out consultations regarding a specific patient in particular from this health area (especially in the transition from one care level to another) but also to refer patients for conducting drug therapy monitoring.
The purpose of this article is to present the requirements, structure and results of the e-Interconsultation platform developed following one year of implementation.
MethodTo carry out the development of the e-Interconsultation platform, a multidisciplinary working group was formed, comprised of three Hospital pharmacists, a primary care pharmacist as the spokesperson for all those belonging to A Coruña’s Integrated Management Area (XXIAC), a Primary Care Administration executive (to whom the primary care pharmacists report) and a professional from the Sub-Directorate of Information Systems and Technologies (a computer engineer). At its first meeting, this working group set out its objectives, working schedule, the computer program requirements, the program structural design, the validation thereof in pilot trials and the implementation.
After setting the working schedule (the intention was to have the system implemented within a six-month period), the necessary requirements of the e-Interconsultation Platform were then determined:
- 1
To allow the access and to identify the PC and HC pharmacists of the health area and a two-way flow of consultations.
- 2
Encoded patient identification to keep confidentiality9.
- 3
To channel and standardize the consultation in terms of their source, primary care or hospital care, as well as the results thereof for their subsequent follow-up.
- 4
To standardize the purpose for which each consultation is made.
- 5
To make it possible to know that status of the consultation, in other words, whether it is pending a solution or has already been solved.
- 6
To have an alerts system so that the people at both ends of the consultation will be aware of its being made.
- 7
To allow for data mining by the different parameters of which it is comprised.
- 8
To be fast, stable, intuitive, simple to access and easy to use.
All of these requirements were conveyed to the computer engineer in the working group for the development of the platform structure. In following, the pilot trials and drills of consultations between hospital care and primary care were carried out. Following their validation, the accesses were created for all of the pharmacists involved (33 in all), informative and training sessions were held and the system was then launched in June 2015 following the approval of the executives in charge of the health area.
ResultsStructure and operationThe computer tools selected as the basis for developing the platform was Microsoft Sharepoint®, which is based on web technology, where the two-way functions between hospital care and primary care were configured. The fields set up are shown in Fig. 1 (HC-to-PC and PC-to-HC online interconsultation forms).


Patient identification is encoded by means of Healthcare card code, making it possible to keep them confidential.
This system has a standardized list of reasons for consultation, subject-based areas and results of the referral, thus making standardized classification and subsequent data mining possible (Fig. 1) and different types of consultation displays, so that each pharmacist can query the status of their consultations, either pending or reviewed.
Each pharmacist access the platform using the corporate user name and password used for the professional applications in the Autonomous Community of Galicia Health System (Sergas). Through the shared collaborative web portal of the Pharmacy Service of the hospital pharmacists and primary care. After registering, the pharmacist selects the source or address of the consultation, given that it will be channeled differently depending on its source: PC to- HC is sent to the pharmacist responsible for each drug therapy area (17 drug therapy areas in all and 21 pharmacists involved), who is the person in charge of managing the interconsultation; HC-to-PC is sent to the pharmacist at the Primary medical center to which the patient in question is assigned (71 centers managed by 12 pharmacists).
Afterward, a new element (new consultation) must then be added, and the online form opens up (Fig. 1) where the required information in each one of the fields must be filled in and then sent.
Once the consultation has been sent, it shows up as a new message on the corporate e-mail of each receiving pharmacist. Several groups and levels of pharmacists have been set for each subject area or Primary medical center so that no consultation is ever left unanswered.
To answer a consultation, the pharmacist must access it via the platform and after opening up the web form again, must edit it to enable the possibility of providing a reply. First of all, the users answering the consultations must identify themselves, then detail their response and the steps taken and then mark a result for the referral of the e-interconsultation from among the possible pre-programmed results or, alternatively, mark the “others” option and detail the result if it does not fit any of those listed above, then click on “reviewed” to close out the e-interconsultation and then lastly click on “send”.
A maximum 72-hour time frame was agreed to for providing a reply according to Regional Healtsystem Regulations10, considering that a large part of the e-interconsultations would be motivated by discrepancies on this regard.
All of the measures can be documented by the pharmacists in the Electronic Clinical History.
ActivityIn June 2016, following one year of the platform having been in operation, a total of 321 e-interconsultations had been made, 110 of which were HC-to-PC referrals, 211 having been PC-to-HC. Table 1 and 2 provide the main results of this study, shown in following:
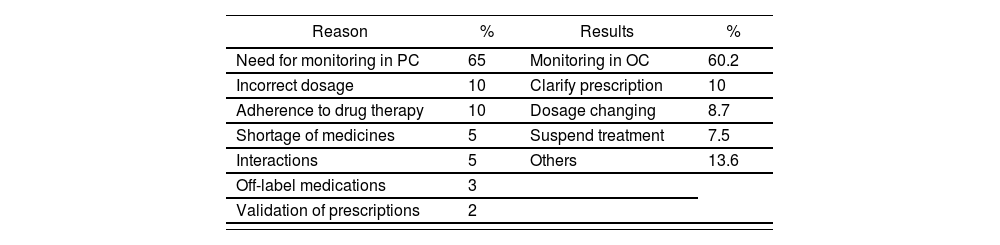
Hospital Pharmacist to Primary Pharmacists e-interconsultations. Total No. = 110
| Reason | % | Results | % |
|---|---|---|---|
| Need for monitoring in PC | 65 | Monitoring in OC | 60.2 |
| Incorrect dosage | 10 | Clarify prescription | 10 |
| Adherence to drug therapy | 10 | Dosage changing | 8.7 |
| Shortage of medicines | 5 | Suspend treatment | 7.5 |
| Interactions | 5 | Others | 13.6 |
| Off-label medications | 3 | ||
| Validation of prescriptions | 2 |
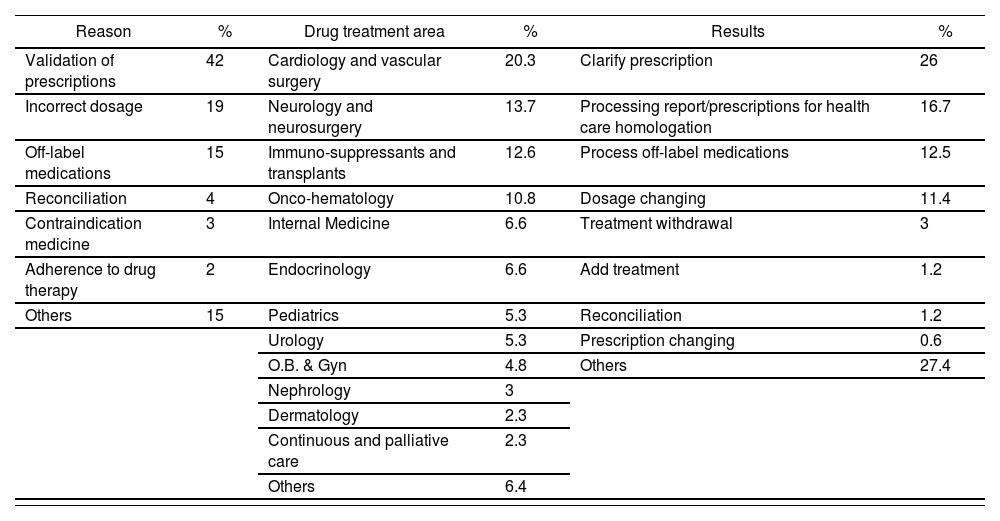
Primary Pharmacists to Hospital Pharmacist e-interconsultations. Total No. = 211
| Reason | % | Drug treatment area | % | Results | % |
|---|---|---|---|---|---|
| Validation of prescriptions | 42 | Cardiology and vascular surgery | 20.3 | Clarify prescription | 26 |
| Incorrect dosage | 19 | Neurology and neurosurgery | 13.7 | Processing report/prescriptions for health care homologation | 16.7 |
| Off-label medications | 15 | Immuno-suppressants and transplants | 12.6 | Process off-label medications | 12.5 |
| Reconciliation | 4 | Onco-hematology | 10.8 | Dosage changing | 11.4 |
| Contraindication medicine | 3 | Internal Medicine | 6.6 | Treatment withdrawal | 3 |
| Adherence to drug therapy | 2 | Endocrinology | 6.6 | Add treatment | 1.2 |
| Others | 15 | Pediatrics | 5.3 | Reconciliation | 1.2 |
| Urology | 5.3 | Prescription changing | 0.6 | ||
| O.B. & Gyn | 4.8 | Others | 27.4 | ||
| Nephrology | 3 | ||||
| Dermatology | 2.3 | ||||
| Continuous and palliative care | 2.3 | ||||
| Others | 6.4 |
A total of 12 Primary Care Pharmacists are on staff at 71 Primary medical centers within this Healthcare area, three of whom have received 45% of the consultations managed by way of this platform (one pharmacist 19% and two pharmacists 13%). The others each covered 3-5%. A total of 10% of the consultations were addressed to all of the PC pharmacists for reasons of information concerning changes in the marketing format of medicines, shortages of medicines or information on medicines.
The major reason for consultation was the need for monitoring in PC (65%), incorrect dosage in some medication (10%) and monitoring adherence to treatment (10%). A total of 60.2% of the referral results requested drug therapy monitoring, 10% clarification of the prescription, 8.7% changes in the dosage of some medication, 7.5% treatment withdrawal and 13.6% taking in other results (off-label treatments, reconciliation or information on medications).
Referrals from Primary Care to Hospital CareA total of 57.4% of these consultations were managed by the hospital pharmacists assigned to 4 of the 16 pre-programmed treatment areas: 20.3% cardiology-heart surgery- vascular surgery, 13.7% neurology, 12.6% transplant-immunosuppression and 10.8% onco-hematology.
The main reason for the consultation was related to Legal Health System authorization of prescriptions of patients being released from the hospital or following an out-of-hospital consultation to the in-hospital medical specialist (42%), followed by the identification of incorrect dosage (19%) and the prescription of off-label medicines (15%).
The main results of the derivation of the consultation were grouped as follows: 26% clarification of the prescription, processing of authorization report and/or prescriptions (16.7%), processing off-label medicine (12.5%) and change in dosage (11.4%); the rest of the consultations (33.4%) included a wide array of results for the derivation.
DiscussionProviding seamless continuous pharmaceutical care with the aid of new integrated information systems and technologies are two of the strategic lines on which the professional development of primary care and hospital care pharmacists who are working in the Spanish Health System must be based. The e-Interconsultation platform which is set out in this study is the first information system presented in Spain which comprises a collaborating mechanism in the transition of patients from one care level to another, which makes it possible to facilitate, standardize and document consultations, derivations and pharmaceutical care interventions. Furthermore, the web platform presented meets the requirements set for its design and is easy to access, simple and user-friendly.
Regarding the results, although we cannot draw any comparative conclusions given that no similar experiences have been published, the total number of interconsultations managed by means of the platform must be said to seem small, considering the total number of patients in the health care area and the activity of the hospital with regard to hospital admissions and outpatient visits made. In this regard, it might be said that the web platform has been implanted for solely one year and despite its being easy to handle, number interconsultations are still being made by telephone, which do not lend themselves to being accounted for on not being recorded or documented. Organizational efforts will have to be made encouraging the use of this tool.
Consultations from HC to PC are due mainly to the need for drug therapy monitoring in primary care of medicines precribed by hospital physicians. This is so due especially to the clinical monitoring required by certain patients who are prescribed a medication at the hospital having clinically-significant interactions with their baseline treatment, medicines which are new on the market or medicines with a narrow therapeutic index. However, the interconsultations from PC to HC are due mainly to the prescription of medicines which are new on the market (such as the new anticoagulants or oral anti-aggregants) or for the monitoring of transplanted patients.
We find the e-Interconsultation platform to be a valid information system for the referral of consultations or patients from one care level to another, which meets all of the requirements initially established and which needs to be used to a greater extent, given its easy handling and the pharmaceutical care documentation provided.
FundingNo funding.
Conflict of interestNo conflict of interest

