

To assess the level of knowledge, perception, and willingness of hospital pharmacy residents in Spain to implement the initiatives of the MAPEX project (Strategic Map for Outpatient Pharmaceutical Care) by the Spanish Society of Hospital Pharmacy in the future, as well as to analyze the influence of outpatient pharmacy rotations on these aspects.
MethodsA four-phase study was conducted: information review and analysis, questionnaire design, survey administration, and final report development. A questionnaire was designed to assess knowledge, perception, and application of MAPEX, as well as experience in outpatient pharmacy rotations. Factorial and bivariate analyses were performed to evaluate the questionnaire structure and identify associations between variables.
ResultsA total of 143 residents participated. Of these, 78.3% had completed an outpatient pharmacy rotation, which was significantly associated with greater knowledge (p = 0.02) and application (p = 0.01) of MAPEX. However, only 15.4% had a high level of knowledge, and 12.6% frequently applied the Capacity-Motivation-Opportunity (CMO) methodology. Although 71.3% positively valued motivational interviewing, only 28% used it frequently. Willingness to implement MAPEX was high (73.4%), reaching 100% among those with a high level of knowledge about the project (p = 0.04). Factor analysis identified six factors explaining 66.8% of the total variance.
ConclusionsHospital pharmacy residents demonstrated a positive perception and a high willingness to implement MAPEX, highlighting the need for its structured integration into specialized training. Outpatient pharmacy rotations significantly improve knowledge and application of the CMO methodology, emphasizing their importance in pharmaceutical care training.
evaluar el grado de conocimiento, percepción y predisposición de los residentes de Farmacia Hospitalaria en España para implementar, en el futuro, las iniciativas del proyecto MAPEX (Mapa Estratégico para la Atención Farmacéutica al Paciente Externo) de la Sociedad Española de Farmacia Hospitalaria, así como analizar la influencia de la rotación en consultas externas en estos aspectos.
Métodosestudio en 4 fases: revisión y análisis de información, diseño del cuestionario, realización de la encuesta y elaboración del informe final. Se diseñó un cuestionario para evaluar el conocimiento, percepción y aplicación de MAPEX, además de la experiencia en rotaciones por consultas externas. Se emplearon análisis factoriales y bivariantes para evaluar la estructura del cuestionario y las asociaciones entre variables.
Resultadosparticiparon 143 residentes. El 78,3% había realizado la rotación en consultas externas, lo que se asoció con un mayor conocimiento (p = 0,02) y aplicación (p = 0,01) de MAPEX. Solo el 15,4% tenía un conocimiento alto, y el 12,6% aplicaba frecuentemente la metodología Capacidad-Motivación-Oportunidad (CMO). Aunque el 71,3% valoró positivamente la entrevista motivacional, solo el 28% la empleaba con frecuencia. La predisposición a implementar MAPEX fue alta (73,4%), alcanzando el 100% entre quienes tenían un conocimiento elevado del proyecto (p = 0,04). El análisis factorial identificó 6 factores que explicaron el 66,8% de la variancia total.
Conclusioneslos residentes muestran una percepción positiva y alta predisposición para aplicar MAPEX, destacando la necesidad de su integración en la formación especializada. La rotación en consultas externas mejora significativamente el conocimiento y la aplicación de la metodología CMO, resaltando su importancia en la capacitación en atención farmacéutica.
The management of chronic diseases emerges as a major challenge in global healthcare systems due to the exponential growth of these diseases and their impact on quality of life.1 This situation has created a need to reconsider healthcare strategies, health policies, and therapeutic approaches in order to address this challenge comprehensively and sustainably.2,3 A thorough understanding of the complexities inherent in healthcare systems, organizational structures, and public health initiatives is essential to ensure an efficient use of resources and enhanced quality of life. A variety of entities are striving to find new strategies that address these challenges from a comprehensive and sustainable approach.4
In the context of Hospital Pharmacy (HP), the steady increase in the number of patients attended in outpatient clinics (OCs), together with resource scarcity, hindered the integration of hospital pharmacists in multidisciplinary teams, resulting in significant variability in patient care. This situation drove the Spanish Society of Hospital Pharmacy (SEFH) to launch a collaborative project to better address these issues.5 In 2014, the SEFH developed the Outpatient Pharmaceutical Care Plan (MAPEX), based on three basic principles: multidisciplinary and multidimensional care, excellence in knowledge, and evaluation of results.
Since then, and following the I Consensus Conference held in 2016, a range of initiatives have been developed to address current challenges.5–7 One of the most remarkable achievements was the redefinition of pharmaceutical care (PC)8 and the creation of the “CMO Model” after Capacity, Motivation and Opportunity. This model met the three major needs identified: personalized care, care based on pharmacotherapeutic goals, and seamless follow-up.9 In line with our commitment to quality of care, a pioneer certification standard, the Q-PEX initiative,10 was developed in 2019.
A comparative analysis of the impact of the project on PC revealed significant improvements both at the national and regional levels.11,12 The II Consensus Conference was held in 2013 to establish priority initiatives to be developed in the 2024–2027 period. One of the initiatives included was “Establishing mechanisms to disseminate MAPEX contents in relation to pharmaceutical care in undergraduate and resident training plans”. It is worth mentioning that the national HP education plan was approved by the National Specialty Committee as far as in 1999.13 Throughout the project, a variety of education and training initiatives have been implemented to disseminate and raise awareness of the activities developed. However, to date, the level of awareness that future pharmacists have of these initiatives and their level of implementation at present and in the future is unknown.
The primary objective of this study is to identify the level of knowledge, perception and willingness of HP residents in Spain to implement MAPEX initiatives in the future. A secondary goal is to determine the structural validity of the questionnaire designed for the purposes of this study.
MethodsThe study was carried out in four phases extending from January to December 2024. The first phase of the project involved organizing the work, analyzing developments and the context, selecting experts, and planning (Phase 1). The second phase entailed drafting the questionnaire (Phase 2), conducting the survey (Phase 3), and finally, preparing the final report and disseminating results (Phase 4).
In Phase 1, an evaluation of project progress between 2015 and 2023 was performed. To this end, a research group was created including HP specialists experienced in PC and MAPEX from different HPs across Spain, along with members of the SEFH Mentorship Working Group and the SEFH representative of residents. This group reviewed and validated the goals, scope, expectations and methods used to design the questionnaire. Additionally, the research group took part in other actions, such as reviewing literature, drafting questionnaire proposals, reaching consensus, reviewing drafts, disseminating the questionnaire and validating the final report.
Phase 2 involved a review and evaluation of relevant literature. To this end, the following MeSH keywords were identified: HP; PC; telepharmacy; training; multidisciplinary integration; and questionnaires. Other useful non-MeSH keywords were added in the literature search for their relation with the MAPEX project. The literature search was restricted to papers published in the last eight years, either in Spanish or English.
Subsequently, an analysis was performed of published questionnaires to gather opinions and experiences with HP initiatives at the national14 and international levels. Additionally, the questionnaires identified were evaluated to determine their validity and viability in our context. Finally, items of interest were grouped into dimensions to characterize the questionnaire, and the final version was established.
Once all the evidence had been gathered, a preliminary questionnaire was drafted, and revisions were made to adjust its semantics. To such end, first, the criteria and items to be included were defined according to the analysis of the literature and in line with previous MAPEX initiatives.
The research group reviewed the preliminary proposal to adjust items, incorporate modifications and develop questionnaire methodology, as well as to reach consensus on these issues and establish a schedule.
A total of 24 questions were defined and classified into four blocks, namely: descriptive questions, MAPEX initiatives, training, and future. Numeric answer options were included. Responses were rated on a 10-point Likert scale and grouped based on their rating: low = 1–4, moderate = 5–7, and high >7. In addition, demographic questions were included, and participants were interrogated about previous rotations in an outpatient HP department. An introduction to the questionnaire was also included to present the project and explain the goals of the survey. Information was included about the time required to complete the questionnaire and its anonymity.
The online questionnaire was disseminated via Google Forms®, which was also used to collect and process information anonymously.
Prior to the final distribution of the questionnaire, a pilot test was carried out in a small group of residents. The purpose was to evaluate the clarity, intelligibility and functionality of questionnaire items, along with identifying potential phrasing errors or ambiguities. A minimum of 20 participants were selected from the centers of the research group. According to the literature, this sample size is adequate for identifying systematic errors in measurement tools. This approach ensures process efficiency and prioritizes error identification, without necessitating a representative statistical analysis at this stage.
Participants anonymously completed the questionnaire on the online platform, mimicking real-world conditions. The pilot group included residents at different levels of training to identify issues relevant to the target population.
Qualitative analysis of pilot-phase feedback led to item rewording and format adjustments before the final version was disseminated. As a result, a clear, intelligible questionnaire appropriate for the primary assessment goal was established.
Eventually, the content of the final questionnaire version was determined, with “How would you assess the level of training provided to pharmacy residents in the methodology and implementation of MAPEX initiatives in your setting?” having been established as the main research question.
The research group agreed to include HP residents of all years of specialty training in the study population, except for first-year residents. Sample size was calculated using Spanish Ministry of Health data regarding HP residency vacancies available on its website and pharmacy practice (PR)-related documents.12 To ensure sample representativeness, the following conditions were established: an expected proportion of 50% (p = 0.5) to maximize variability, a 95% confidence interval, and 5% sampling error.
In phase 3, the data collection period started in October 2024. The online questionnaire was distributed through the SEFH official channels, reaching all eligible candidates. A transparent, non-competitive recruitment process was conducted at hospitals across all levels of care in all autonomous communities in Spain where PH residency plans were available. To ensure an adequate sample size, the questionnaire could not be submitted unless all questions were answered.
In phase 4, a descriptive analysis of the baseline characteristics of participants was performed. Categorical variables were expressed as absolute frequencies and percentages. Bivariate Chi-square analyses were conducted to examine associations between outpatient rotation participation, questionnaire responses, and MAPEX project knowledge. Assigning a high score to the first two questions indicated a high level of understanding of MAPEX.
For the secondary objective, the structural validity of the questionnaire was evaluated by principal component factor analysis with varimax rotation. The suitability of the data for factor analysis was assessed via the Kaiser-Meyer-Olkin (KMO) measure and Bartlett's Test of Sphericity. Factors with eigenvalues >1 were retained. A scree plot was used to determine the optimal number of factors. Factor loadings >0.6 were indicated as representativeness. All analyses were performed using the SPSS version 26 software package (IBM Corp., Armonk, NY, USA).
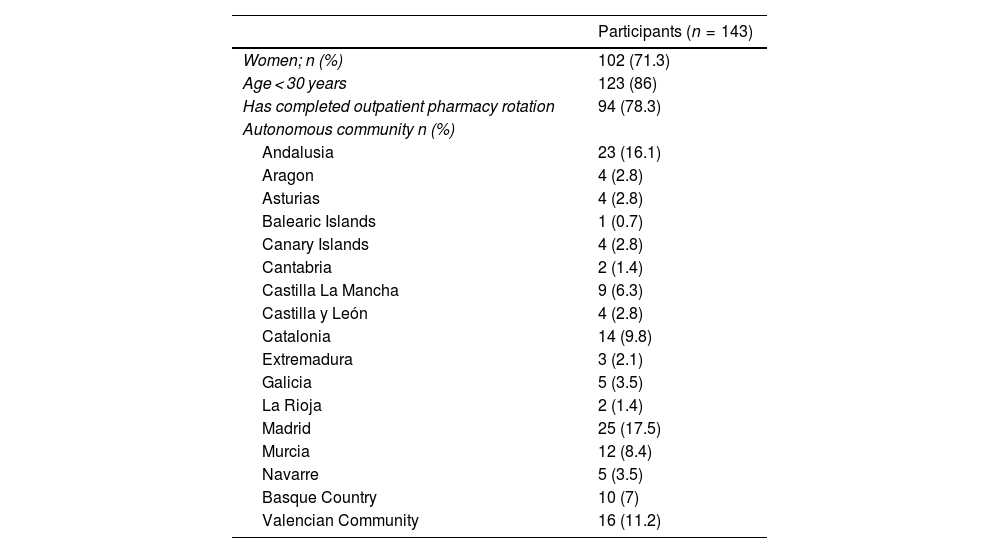
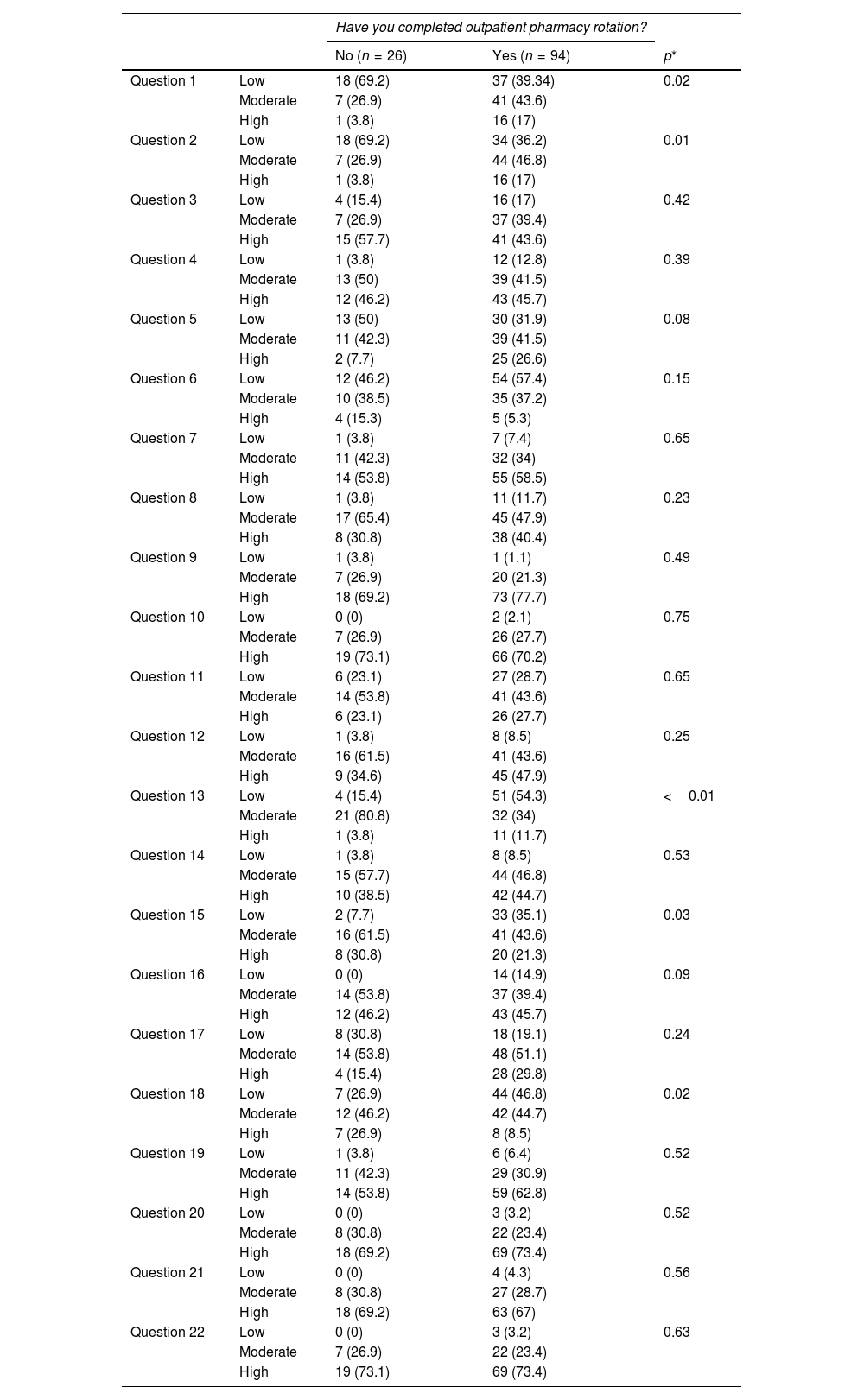
ResultsA total of 143 PRs completed the survey. Most participants were female (71.3%), of whom 86% were younger than 30. The geographic distribution was representative of all autonomous communities, which guaranteed sample diversity. As many as 78.3% of respondents had already completed their outpatient pharmacy rotation period (Table 1). In total, 15.4% and 42.7% of participants had a high and a low level of understanding of the MAPEX project, respectively. MAPEX knowledge differed significantly between participants who had completed the outpatient HP rotation and those who had not (p = 0.02). Thus, the residents having completed the outpatient HP rotation were more familiarized with the MAPEX project (17% vs. 3.8%) (Table 2).
Baseline characteristics of study participants.
| Participants (n = 143) | |
|---|---|
| Women; n (%) | 102 (71.3) |
| Age < 30 years | 123 (86) |
| Has completed outpatient pharmacy rotation | 94 (78.3) |
| Autonomous community n (%) | |
| Andalusia | 23 (16.1) |
| Aragon | 4 (2.8) |
| Asturias | 4 (2.8) |
| Balearic Islands | 1 (0.7) |
| Canary Islands | 4 (2.8) |
| Cantabria | 2 (1.4) |
| Castilla La Mancha | 9 (6.3) |
| Castilla y León | 4 (2.8) |
| Catalonia | 14 (9.8) |
| Extremadura | 3 (2.1) |
| Galicia | 5 (3.5) |
| La Rioja | 2 (1.4) |
| Madrid | 25 (17.5) |
| Murcia | 12 (8.4) |
| Navarre | 5 (3.5) |
| Basque Country | 10 (7) |
| Valencian Community | 16 (11.2) |
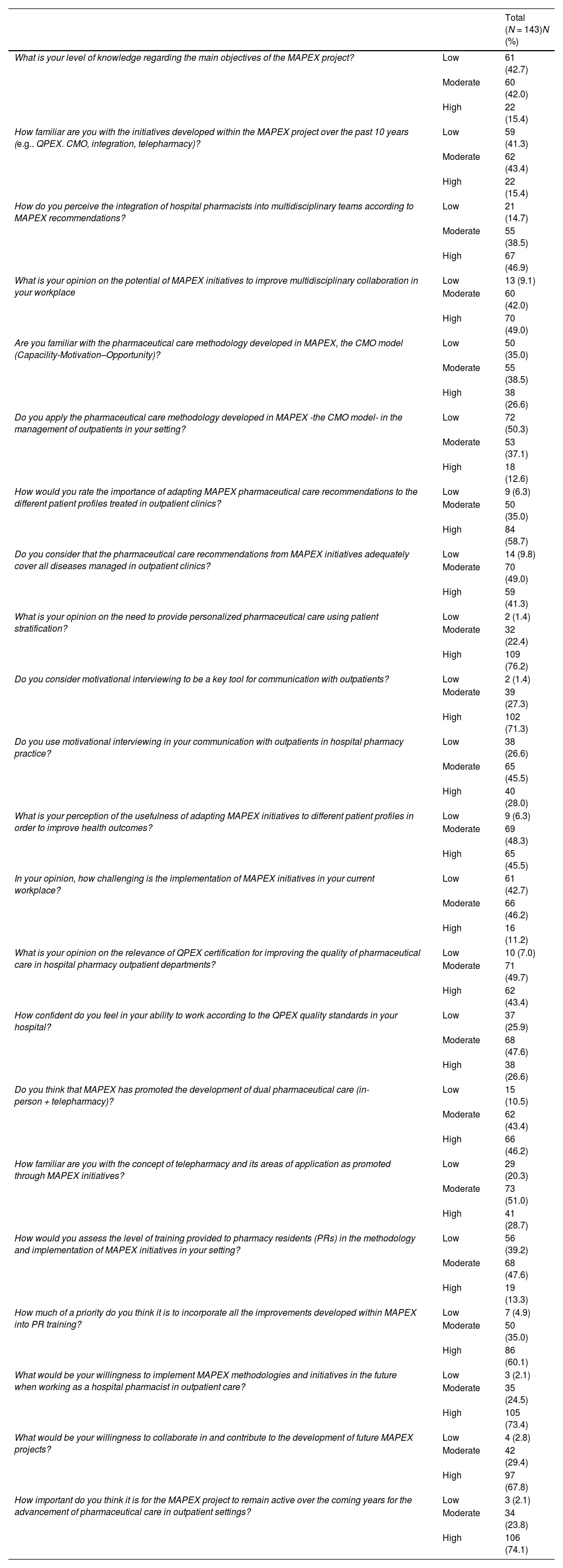
Questionnaire Responses.
| Total (N = 143)N (%) | ||
|---|---|---|
| What is your level of knowledge regarding the main objectives of the MAPEX project? | Low | 61 (42.7) |
| Moderate | 60 (42.0) | |
| High | 22 (15.4) | |
| How familiar are you with the initiatives developed within the MAPEX project over the past 10 years (e.g.. QPEX. CMO, integration, telepharmacy)? | Low | 59 (41.3) |
| Moderate | 62 (43.4) | |
| High | 22 (15.4) | |
| How do you perceive the integration of hospital pharmacists into multidisciplinary teams according to MAPEX recommendations? | Low | 21 (14.7) |
| Moderate | 55 (38.5) | |
| High | 67 (46.9) | |
| What is your opinion on the potential of MAPEX initiatives to improve multidisciplinary collaboration in your workplace | Low | 13 (9.1) |
| Moderate | 60 (42.0) | |
| High | 70 (49.0) | |
| Are you familiar with the pharmaceutical care methodology developed in MAPEX, the CMO model (Capacility-Motivation–Opportunity)? | Low | 50 (35.0) |
| Moderate | 55 (38.5) | |
| High | 38 (26.6) | |
| Do you apply the pharmaceutical care methodology developed in MAPEX -the CMO model- in the management of outpatients in your setting? | Low | 72 (50.3) |
| Moderate | 53 (37.1) | |
| High | 18 (12.6) | |
| How would you rate the importance of adapting MAPEX pharmaceutical care recommendations to the different patient profiles treated in outpatient clinics? | Low | 9 (6.3) |
| Moderate | 50 (35.0) | |
| High | 84 (58.7) | |
| Do you consider that the pharmaceutical care recommendations from MAPEX initiatives adequately cover all diseases managed in outpatient clinics? | Low | 14 (9.8) |
| Moderate | 70 (49.0) | |
| High | 59 (41.3) | |
| What is your opinion on the need to provide personalized pharmaceutical care using patient stratification? | Low | 2 (1.4) |
| Moderate | 32 (22.4) | |
| High | 109 (76.2) | |
| Do you consider motivational interviewing to be a key tool for communication with outpatients? | Low | 2 (1.4) |
| Moderate | 39 (27.3) | |
| High | 102 (71.3) | |
| Do you use motivational interviewing in your communication with outpatients in hospital pharmacy practice? | Low | 38 (26.6) |
| Moderate | 65 (45.5) | |
| High | 40 (28.0) | |
| What is your perception of the usefulness of adapting MAPEX initiatives to different patient profiles in order to improve health outcomes? | Low | 9 (6.3) |
| Moderate | 69 (48.3) | |
| High | 65 (45.5) | |
| In your opinion, how challenging is the implementation of MAPEX initiatives in your current workplace? | Low | 61 (42.7) |
| Moderate | 66 (46.2) | |
| High | 16 (11.2) | |
| What is your opinion on the relevance of QPEX certification for improving the quality of pharmaceutical care in hospital pharmacy outpatient departments? | Low | 10 (7.0) |
| Moderate | 71 (49.7) | |
| High | 62 (43.4) | |
| How confident do you feel in your ability to work according to the QPEX quality standards in your hospital? | Low | 37 (25.9) |
| Moderate | 68 (47.6) | |
| High | 38 (26.6) | |
| Do you think that MAPEX has promoted the development of dual pharmaceutical care (in-person + telepharmacy)? | Low | 15 (10.5) |
| Moderate | 62 (43.4) | |
| High | 66 (46.2) | |
| How familiar are you with the concept of telepharmacy and its areas of application as promoted through MAPEX initiatives? | Low | 29 (20.3) |
| Moderate | 73 (51.0) | |
| High | 41 (28.7) | |
| How would you assess the level of training provided to pharmacy residents (PRs) in the methodology and implementation of MAPEX initiatives in your setting? | Low | 56 (39.2) |
| Moderate | 68 (47.6) | |
| High | 19 (13.3) | |
| How much of a priority do you think it is to incorporate all the improvements developed within MAPEX into PR training? | Low | 7 (4.9) |
| Moderate | 50 (35.0) | |
| High | 86 (60.1) | |
| What would be your willingness to implement MAPEX methodologies and initiatives in the future when working as a hospital pharmacist in outpatient care? | Low | 3 (2.1) |
| Moderate | 35 (24.5) | |
| High | 105 (73.4) | |
| What would be your willingness to collaborate in and contribute to the development of future MAPEX projects? | Low | 4 (2.8) |
| Moderate | 42 (29.4) | |
| High | 97 (67.8) | |
| How important do you think it is for the MAPEX project to remain active over the coming years for the advancement of pharmaceutical care in outpatient settings? | Low | 3 (2.1) |
| Moderate | 34 (23.8) | |
| High | 106 (74.1) | |
Scale scores: low = 1–4, moderate = 5–7, high > 7.
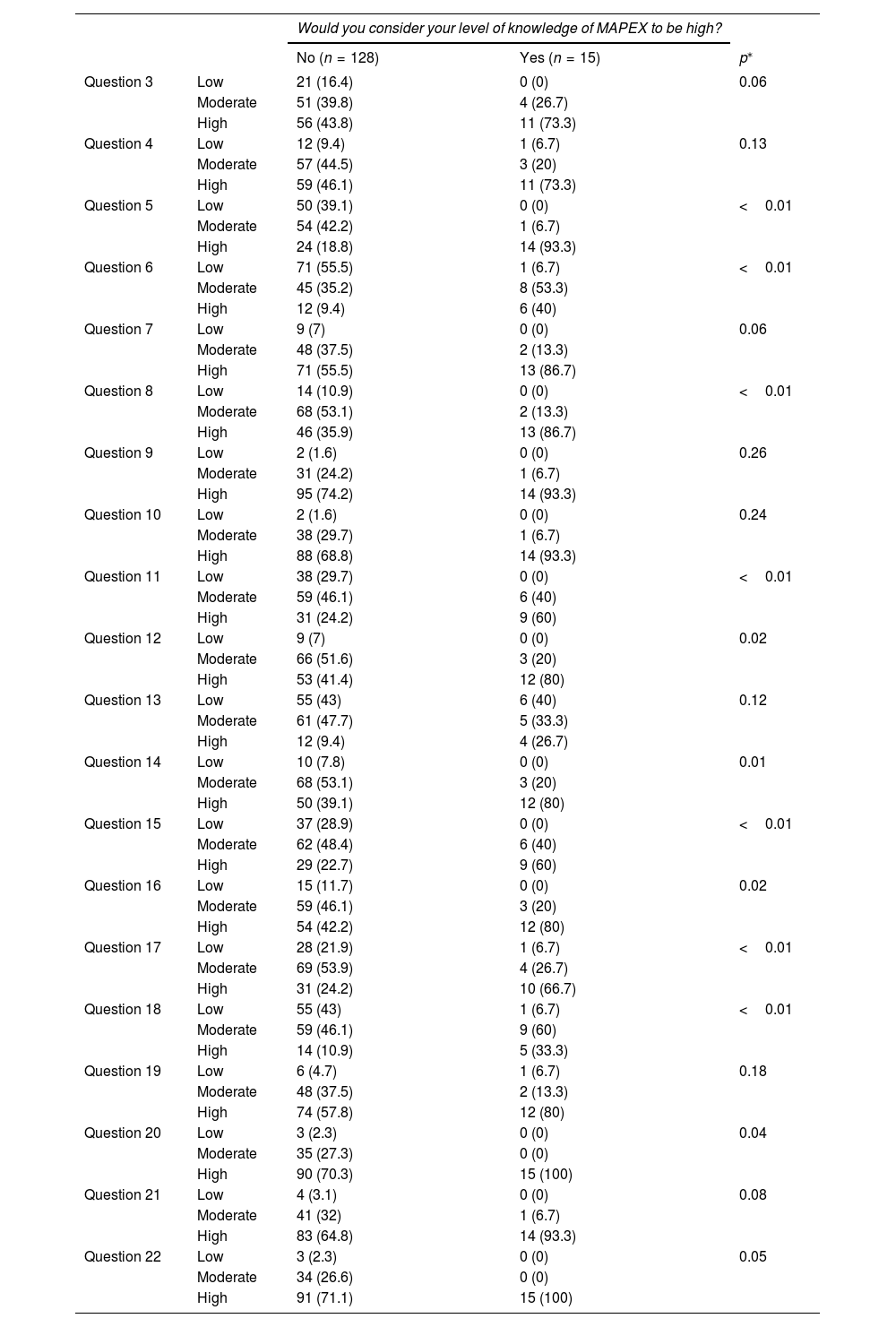
With respect to knowledge and adoption of the CMO methodology, only 12.6% of participants reported using it frequently, with participants having completed rotation showing a higher level of familiarity with this method (p = 0.01). The use of CMO was more frequent among participants with a high understanding of MAPEX (40.0% vs. 9.4%, p < 0.01). Participants considered motivational interviewing to be highly relevant (71.3%), albeit only 28.0% used it frequently. Residents strongly familiar with MAPEX were more likely to use motivational interviewing (60.0% vs. 24.2%, p < 0.01) (Table 3).
Results of bivariate analyses based on outpatient HP rotation completion status.
| Have you completed outpatient pharmacy rotation? | ||||
|---|---|---|---|---|
| No (n = 26) | Yes (n = 94) | p⁎ | ||
| Question 1 | Low | 18 (69.2) | 37 (39.34) | 0.02 |
| Moderate | 7 (26.9) | 41 (43.6) | ||
| High | 1 (3.8) | 16 (17) | ||
| Question 2 | Low | 18 (69.2) | 34 (36.2) | 0.01 |
| Moderate | 7 (26.9) | 44 (46.8) | ||
| High | 1 (3.8) | 16 (17) | ||
| Question 3 | Low | 4 (15.4) | 16 (17) | 0.42 |
| Moderate | 7 (26.9) | 37 (39.4) | ||
| High | 15 (57.7) | 41 (43.6) | ||
| Question 4 | Low | 1 (3.8) | 12 (12.8) | 0.39 |
| Moderate | 13 (50) | 39 (41.5) | ||
| High | 12 (46.2) | 43 (45.7) | ||
| Question 5 | Low | 13 (50) | 30 (31.9) | 0.08 |
| Moderate | 11 (42.3) | 39 (41.5) | ||
| High | 2 (7.7) | 25 (26.6) | ||
| Question 6 | Low | 12 (46.2) | 54 (57.4) | 0.15 |
| Moderate | 10 (38.5) | 35 (37.2) | ||
| High | 4 (15.3) | 5 (5.3) | ||
| Question 7 | Low | 1 (3.8) | 7 (7.4) | 0.65 |
| Moderate | 11 (42.3) | 32 (34) | ||
| High | 14 (53.8) | 55 (58.5) | ||
| Question 8 | Low | 1 (3.8) | 11 (11.7) | 0.23 |
| Moderate | 17 (65.4) | 45 (47.9) | ||
| High | 8 (30.8) | 38 (40.4) | ||
| Question 9 | Low | 1 (3.8) | 1 (1.1) | 0.49 |
| Moderate | 7 (26.9) | 20 (21.3) | ||
| High | 18 (69.2) | 73 (77.7) | ||
| Question 10 | Low | 0 (0) | 2 (2.1) | 0.75 |
| Moderate | 7 (26.9) | 26 (27.7) | ||
| High | 19 (73.1) | 66 (70.2) | ||
| Question 11 | Low | 6 (23.1) | 27 (28.7) | 0.65 |
| Moderate | 14 (53.8) | 41 (43.6) | ||
| High | 6 (23.1) | 26 (27.7) | ||
| Question 12 | Low | 1 (3.8) | 8 (8.5) | 0.25 |
| Moderate | 16 (61.5) | 41 (43.6) | ||
| High | 9 (34.6) | 45 (47.9) | ||
| Question 13 | Low | 4 (15.4) | 51 (54.3) | <0.01 |
| Moderate | 21 (80.8) | 32 (34) | ||
| High | 1 (3.8) | 11 (11.7) | ||
| Question 14 | Low | 1 (3.8) | 8 (8.5) | 0.53 |
| Moderate | 15 (57.7) | 44 (46.8) | ||
| High | 10 (38.5) | 42 (44.7) | ||
| Question 15 | Low | 2 (7.7) | 33 (35.1) | 0.03 |
| Moderate | 16 (61.5) | 41 (43.6) | ||
| High | 8 (30.8) | 20 (21.3) | ||
| Question 16 | Low | 0 (0) | 14 (14.9) | 0.09 |
| Moderate | 14 (53.8) | 37 (39.4) | ||
| High | 12 (46.2) | 43 (45.7) | ||
| Question 17 | Low | 8 (30.8) | 18 (19.1) | 0.24 |
| Moderate | 14 (53.8) | 48 (51.1) | ||
| High | 4 (15.4) | 28 (29.8) | ||
| Question 18 | Low | 7 (26.9) | 44 (46.8) | 0.02 |
| Moderate | 12 (46.2) | 42 (44.7) | ||
| High | 7 (26.9) | 8 (8.5) | ||
| Question 19 | Low | 1 (3.8) | 6 (6.4) | 0.52 |
| Moderate | 11 (42.3) | 29 (30.9) | ||
| High | 14 (53.8) | 59 (62.8) | ||
| Question 20 | Low | 0 (0) | 3 (3.2) | 0.52 |
| Moderate | 8 (30.8) | 22 (23.4) | ||
| High | 18 (69.2) | 69 (73.4) | ||
| Question 21 | Low | 0 (0) | 4 (4.3) | 0.56 |
| Moderate | 8 (30.8) | 27 (28.7) | ||
| High | 18 (69.2) | 63 (67) | ||
| Question 22 | Low | 0 (0) | 3 (3.2) | 0.63 |
| Moderate | 7 (26.9) | 22 (23.4) | ||
| High | 19 (73.1) | 69 (73.4) | ||
Scale scores: low = 1–4, moderate = 5–7, high > 7.
Finally, in relation to participants' perception and willingness to implement MAPEX in the future, 73.4% showed a high willingness, reaching 100% among participants with a high level of knowledge (p = 0.04) (Table 4).
Results of bivariate analysis by level of knowledge about MAPEX.
| Would you consider your level of knowledge of MAPEX to be high? | ||||
|---|---|---|---|---|
| No (n = 128) | Yes (n = 15) | p⁎ | ||
| Question 3 | Low | 21 (16.4) | 0 (0) | 0.06 |
| Moderate | 51 (39.8) | 4 (26.7) | ||
| High | 56 (43.8) | 11 (73.3) | ||
| Question 4 | Low | 12 (9.4) | 1 (6.7) | 0.13 |
| Moderate | 57 (44.5) | 3 (20) | ||
| High | 59 (46.1) | 11 (73.3) | ||
| Question 5 | Low | 50 (39.1) | 0 (0) | <0.01 |
| Moderate | 54 (42.2) | 1 (6.7) | ||
| High | 24 (18.8) | 14 (93.3) | ||
| Question 6 | Low | 71 (55.5) | 1 (6.7) | <0.01 |
| Moderate | 45 (35.2) | 8 (53.3) | ||
| High | 12 (9.4) | 6 (40) | ||
| Question 7 | Low | 9 (7) | 0 (0) | 0.06 |
| Moderate | 48 (37.5) | 2 (13.3) | ||
| High | 71 (55.5) | 13 (86.7) | ||
| Question 8 | Low | 14 (10.9) | 0 (0) | <0.01 |
| Moderate | 68 (53.1) | 2 (13.3) | ||
| High | 46 (35.9) | 13 (86.7) | ||
| Question 9 | Low | 2 (1.6) | 0 (0) | 0.26 |
| Moderate | 31 (24.2) | 1 (6.7) | ||
| High | 95 (74.2) | 14 (93.3) | ||
| Question 10 | Low | 2 (1.6) | 0 (0) | 0.24 |
| Moderate | 38 (29.7) | 1 (6.7) | ||
| High | 88 (68.8) | 14 (93.3) | ||
| Question 11 | Low | 38 (29.7) | 0 (0) | <0.01 |
| Moderate | 59 (46.1) | 6 (40) | ||
| High | 31 (24.2) | 9 (60) | ||
| Question 12 | Low | 9 (7) | 0 (0) | 0.02 |
| Moderate | 66 (51.6) | 3 (20) | ||
| High | 53 (41.4) | 12 (80) | ||
| Question 13 | Low | 55 (43) | 6 (40) | 0.12 |
| Moderate | 61 (47.7) | 5 (33.3) | ||
| High | 12 (9.4) | 4 (26.7) | ||
| Question 14 | Low | 10 (7.8) | 0 (0) | 0.01 |
| Moderate | 68 (53.1) | 3 (20) | ||
| High | 50 (39.1) | 12 (80) | ||
| Question 15 | Low | 37 (28.9) | 0 (0) | <0.01 |
| Moderate | 62 (48.4) | 6 (40) | ||
| High | 29 (22.7) | 9 (60) | ||
| Question 16 | Low | 15 (11.7) | 0 (0) | 0.02 |
| Moderate | 59 (46.1) | 3 (20) | ||
| High | 54 (42.2) | 12 (80) | ||
| Question 17 | Low | 28 (21.9) | 1 (6.7) | <0.01 |
| Moderate | 69 (53.9) | 4 (26.7) | ||
| High | 31 (24.2) | 10 (66.7) | ||
| Question 18 | Low | 55 (43) | 1 (6.7) | <0.01 |
| Moderate | 59 (46.1) | 9 (60) | ||
| High | 14 (10.9) | 5 (33.3) | ||
| Question 19 | Low | 6 (4.7) | 1 (6.7) | 0.18 |
| Moderate | 48 (37.5) | 2 (13.3) | ||
| High | 74 (57.8) | 12 (80) | ||
| Question 20 | Low | 3 (2.3) | 0 (0) | 0.04 |
| Moderate | 35 (27.3) | 0 (0) | ||
| High | 90 (70.3) | 15 (100) | ||
| Question 21 | Low | 4 (3.1) | 0 (0) | 0.08 |
| Moderate | 41 (32) | 1 (6.7) | ||
| High | 83 (64.8) | 14 (93.3) | ||
| Question 22 | Low | 3 (2.3) | 0 (0) | 0.05 |
| Moderate | 34 (26.6) | 0 (0) | ||
| High | 91 (71.1) | 15 (100) | ||
Scale scores: low = 1–4, moderate = 5–7, high > 7.
On another note, the exploratory factor analysis conducted to explore the structural validity of the questionnaire identified a consistent latent structure composed of six factors aggregately explaining 66.8% of the total variance in responses. The KMO sample suitability test yielded a value of 0.828, thus indicating an excellent partial correlation between items and the suitability of factor analysis in this dataset. Likewise, Bartlett's Test of Sphericity showed significance (χ2 = 1373.617, p < 0.001), which confirmed that correlations between variables warrant the use of a factor model.
The scree plot (Fig. 1) included the values obtained for each component, showing a significant reduction after Factor 6. This turning point supports the selection of a six-factor structure as the most suitable for describing the underlying dimensions of the questionnaire. Each factor represents a specific dimension of the phenomenon tested. Factor 1 stood out with high factor loadings in the questions related to general perceptions and technical competences of clinical rotation (P13, P21 and P22, with loadings >0.7). Factor 2 encompassed items associated with practical skills and specific technical competences (P2, P3 and P9, with loadings >0.6). The remaining factors provide a broader perspective. Factor 3 is associated with the applicability of knowledge; Factor 4 with interpersonal skills and teamwork; Factor 5 with confidence and autonomy in decision-making; and Factor 6 with motivation and satisfaction with training. This structure provides a comprehensive understanding of the latent components investigated.

The consistency of the model was also confirmed by communalities, which ranged from 0.457 to 0.865, with most variables exceeding the 0.6 threshold, which indicates that they are adequately represented by the factors identified.
DiscussionTo the best of our knowledge, this is the first study to assess the level of knowledge, perception and predisposition of hospital pharmacy residents in Spain regarding the MAPEX project. The results obtained provide a comprehensive perspective of the current impact of this strategy on pharmacy residents.
Completion of outpatient pharmacy practice rotation was significantly associated with a higher level of knowledge and adoption of the method and initiatives developed, which supports its role as a key component in PR training and education. This finding is consistent with previous studies underscoring the relevance of direct clinical experiences in consolidating technical skills and improving the implementation of innovative healthcare models.15,16 However, the variability observed among residents suggests a lack of homogeneity regarding their knowledge of MAPEX. Discrepancies could stem from structural and organizational differences across HP departments. These differences may also stem from variability in the training of HP supervisors responsible for conveying the core instructional components of pharmacy practice rotations.
Incorporating standardized practice rotation plans into the future national PR rotation plan would help overcome these limitations and promote greater uniformity in education and training. In this sense, international initiatives such as the ASHP Practice Advancement Initiative 2030 promote the integration of structured clinical experiences as a strategy to improve training among hospital pharmacists in early training stages.4 This approach should be adopted in Spain to enhance the impact of MAPEX.
With regard to specific initiatives, although respondents considered motivational interviewing relevant, they rarely apply this strategy. This unbalance illustrates a gap between theory and practice. The observed imbalance reveals a gap between theory and practice, likely attributable to inadequate communication training during PR and aligned with the ongoing transition from a drug-centered approach toward a patient-centered model of care. Pharmacy residency plans should incorporate specific modules on motivational interviewing, such as those implemented in multidimensional models of care, as these have been shown to improve treatment adherence and health outcomes.17
The observed association between greater knowledge of MAPEX and an increased willingness to apply it in future practice underscores the need to integrate targeted content from the most recent initiatives into PR programs. This recommendation is consistent with the principle of continuous learning, widely recognized as essential for maintaining professional competence in evolving healthcare environments.18,19 Moreover, the progressive implementation of the QPEX certification standard in Spanish hospitals may serve as an additional incentive to promote the adoption of quality-oriented practices, as has been reported in comparable experiences across other European countries.20
The establishment of MAPEX as a standard of outpatient care has the potential to improve health outcomes, foster multidisciplinary collaboration, and optimize resource utilization, in line with the vision of hospitals of the future.21 Nevertheless, to ensure its successful integration, it is crucial to address identified barriers, dispel misconceptions and false beliefs, and reduce variability in training access and the lack of standardization.22 Additionally, the development of technologies enabling the implementation of the CMO model could expedite its adoption, in line with other healthcare settings.23
Our study has some limitations. Firstly, the use of a novel, anonymous, self-administered questionnaire may have produced social or professional-desirability bias or interpretation bias by participants, potentially affecting the accuracy of responses. Secondly, data collection was conducted exclusively online, which may have limited participation among less motivated residents. The cross-sectional design of the study precludes the establishment of causal relationships between the variables analyzed, restricting interpretation to the identification of significant associations. Finally, although broad sampling was attempted, the final sample size may not fully reflect the diversity of training and organizational contexts of PR programs across Spain, particularly in regions with lower representation. Despite these limitations, the study also demonstrated several methodological strengths. The structural validation of the questionnaire ensured internal consistency and allowed for the identification of key dimensions related to the knowledge, perception, and implementation of MAPEX. This tool could be replicated in future research to monitor progress and assess long-term impact, thereby contributing to a broader understanding of both educational and clinical needs.
In conclusion, this study identified variable levels of knowledge, generally favorable perceptions, and a high willingness among FIR residents to participate in the future implementation of MAPEX initiatives. These findings suggest promising prospects for the expansion and sustainability of MAPEX as a guiding framework for ambulatory care in specialized settings in Spain over the coming years.
Contribution to the scientific literatureThis study represents a significant contribution to the field of Hospital Pharmacy as it is the first to assess the level of knowledge, perceptions, and willingness of hospital pharmacy residents in Spain with respect to the MAPEX project (Strategic Outpatient Pharmaceutical care Plan) of the Spanish Society of Hospital Pharmacy. The findings underscore the value of outpatient clinic rotations in consolidating key competencies, as well as the need to standardize and expand training in pharmaceutical care within the specialty program. Furthermore, the results reflect a favorable perception of the initiatives developed under MAPEX, particularly in areas such as multidisciplinary integration and anticipatory patient care. Overall, this research provides evidence supporting the relevance of the initiative in both training and clinical practice, highlighting its potential to enhance the quality of pharmaceutical care. The data generated may inform strategic planning and the implementation of harmonized educational policies on MAPEX, thereby contributing to the advancement of pharmaceutical practice and the long-term sustainability of healthcare delivery.
Ethic considerationsThe study protocol was reviewed and approved by the Ethics Committee Sevilla Sur (SICEIA-2024-001533).
CRediT authorship contribution statementMaría Alfonsín Lara: Writing – review & editing, Visualization, Validation, Methodology. Vera Áreas del Águila: Writing – review & editing, Visualization, Validation, Methodology, Investigation, Conceptualization. Enrique Contreras Macías: Writing – review & editing, Writing – original draft, Validation, Formal analysis, Data curation. Almudena Mancebo González: Writing – review & editing, Validation, Investigation, Data curation, Conceptualization. Beatriz Martínez Castro: Writing – review & editing, Visualization, Validation, Methodology, Investigation. Covadonga Pérez Menéndez-Conde: Writing – review & editing, Visualization, Validation, Project administration, Investigation, Conceptualization. Patricia Sanmartín Fenollera: Writing – review & editing, Visualization, Validation, Investigation. Ramón Morillo-Verdugo: Writing – review & editing, Writing – original draft, Visualization, Validation, Supervision, Project administration, Investigation, Conceptualization.
AuthorshipAll authors contributed equally to the inception and design of the study. Ramón Morillo-Verdugo prepared the manuscript. All authors reviewed and approved the final version of the manuscript for submission.
FundingThis study did not receive any funding.
The authors declare no conflicts of interest associated with this publication.
Thanks to all study participants. Thanks to Dr. Manuel Vélez Díaz-Pallares for his unvaluable collaboration in the development of the project.

