
The CMO (Capability-Motivation-Opportunity) methodology is an innovative pharmaceutical care model designed to improve the quality of care for people living with HIV (PLWH). This approach evaluates the knowledge, perception, and willingness to implement the methodology among specialist physicians in Spain.
MethodsThis observational and descriptive study utilized a validated questionnaire distributed among clinicians involved in the care of PLWH. The survey assessed their knowledge and perception of the methodology. Associations between variables were analyzed using bivariate tests.
ResultsThirty physicians participated. Sixty percent reported moderate-to-high knowledge of the methodology, correlating with a positive perception of its clinical relevance (p = 0.02). Motivational interviewing and remote follow-up were identified as key tools.
ConclusionKnowledge of the CMO methodology is limited but positively valued. Its association with improved quality of health care underscores the importance of strategies to enhance its dissemination and adoption in clinical practice.
La metodología CMO (Capacidad-Motivación-Oportunidad) es un modelo innovador de atención farmacéutica diseñado para mejorar la calidad asistencial en las personas que viven con VIH (PVV). Este enfoque analiza el conocimiento, percepción y predisposición para su implementación entre médicos especialistas en España.
MétodosEstudio observacional y descriptivo que empleó un cuestionario validado, distribuido entre clínicos dedicados a PVV, que exploró el conocimiento y la percepción sobre la metodología. Las asociaciones entre variables se evaluaron mediante pruebas bivariantes.
ResultadosSe incluyeron 30 médicos. Un 60% reportó un conocimiento moderado-alto de la metodología, asociándolo con una percepción positiva por su relevancia clínica (p = 0,02). La entrevista motivacional y el seguimiento remoto fueron valorados como herramientas clave.
ConclusiónEl conocimiento de la metodología CMO es limitado, pero positivamente valorado. Su asociación con la mejora de la calidad de la atención sanitaria subraya la importancia de implementar estrategias para fomentar su difusión y adopción en la práctica clínica.
The optimal clinical outcomes of antiretroviral therapy (ART) have transformed HIV infection into a chronic condition, presenting significant challenges associated with aging, such as the emergence of age-related comorbidities and polypharmacy.1 In this context, one of the priorities in the care of people living with HIV (PLWH) is the development of interventions aimed at improving health outcomes, particularly quality of life.2
In the field of Hospital Pharmacy (HP), the increasing number of patients served in outpatient clinics, together with the evolving profile of PLWH, also poses challenges. These challenges are influenced by significant variability in care delivery, prompting the Spanish Society of Hospital Pharmacy (SEFH) to implement initiatives that enable a structured, collaborative, and consensus-driven response among healthcare professionals.3 To this end, in 2014, the project “Strategic Map for Pharmaceutical Care for Outpatients” (MAPEX-SEFH) was launched, focusing on multidisciplinary and multidimensional pharmaceutical care (PC) characterized by excellence in knowledge, evaluation of outcomes, and an anticipatory approach to future needs.3
One of the most significant advances of this project has been the redefinition of the concept of PC itself.4 Within this framework, the capacity-motivation-opportunity (CMO) Pharmaceutical Care Model was designed to address three major identified care needs: individualized care based on a multidimensional approach; a professional orientation focused on achieving pharmacotherapeutic objectives; and longitudinal monitoring to ensure continuity of care.5
Since its development in 2016, the CMO methodology has proven to be an effective strategy for improving clinical outcomes and the quality of life of PLWH, as evidenced by various high-impact multicenter studies.6 This methodology has been associated with significant improvements in patient experience, adherence to ART, virological control, and management of comorbidities.7 These outcomes support its adoption as a reference standard for care, grounded in multidisciplinary collaboration.8 However, its implementation has not been uniform across the national territory due to various factors, including limited awareness among other healthcare professionals regarding the potential health benefits it can offer.8,9
The objective of this study was to evaluate the level of knowledge, perception, and willingness to implement the CMO methodology among medical specialists caring for PLWH in Spain.
MethodsThis observational, descriptive, and cross-sectional study was conducted in two phases between June and December 2024.
In the first phase, a specific questionnaire was designed based on a systematic review of the scientific literature related to the CMO methodology and its applicability in healthcare contexts. The questionnaire included items aimed at exploring key dimensions such as knowledge of the methodology, its perceived relevance, and the willingness to adopt it. Content validation was performed by an expert committee to ensure the relevance and clarity of the selected items. Responses were classified into three categories: low,1–4 moderate,5–7 and high.7–10
The second phase involved anonymous data collection. The questionnaire was distributed through SEFH's mailing list to its members, who were encouraged to share the invitation to participate with clinicians at their respective centers. The questionnaire was hosted on an electronic platform and distributed via the SEFH mailing list, with participation restricted to physicians who received a prior invitation to ensure a representative focus on the target population.
The target population consisted of medical specialists actively managing PLWH in Spain. Inclusion criteria were limited to physicians who completed the questionnaire in its entirety, while those with incomplete responses or who did not meet the established criteria were excluded.
A descriptive analysis of the participants' baseline characteristics was performed, with categorical variables expressed as absolute frequencies and percentages. Additionally, bivariate analyses were conducted to assess associations among physicians with knowledge of the CMO model, using the Chi-square test or Fisher's exact test, as appropriate. A high level of knowledge was defined as responses indicating moderate-to-high familiarity in the question, “How would you rate your knowledge of the CMO methodology?” Statistical significance was set at p < 0.05. The analysis was performed using SPSS statistical software, version 26 (IBM Corp., Armonk, NY, USA).
The study protocol and all relevant documentation were reviewed and approved by the South Seville Research Ethics Committee (code SICEIA-2024-000342).
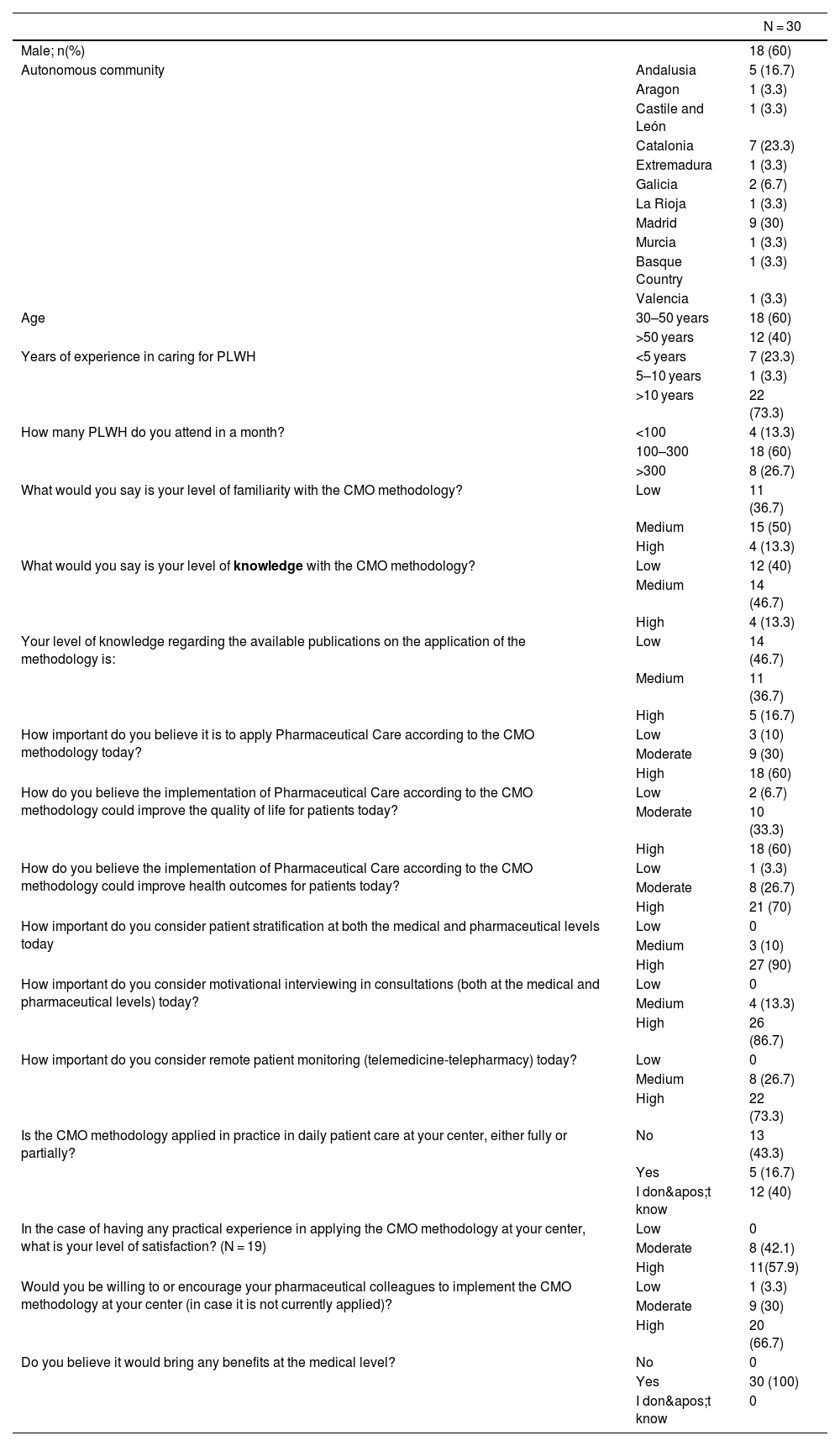
ResultsA total of 30 participants were included, 60% of whom were male. Table 1 summarizes the baseline characteristics and questionnaire responses.
Baseline Characteristics of Study Participants and Questionnaire Responses.
| N = 30 | ||
|---|---|---|
| Male; n(%) | 18 (60) | |
| Autonomous community | Andalusia | 5 (16.7) |
| Aragon | 1 (3.3) | |
| Castile and León | 1 (3.3) | |
| Catalonia | 7 (23.3) | |
| Extremadura | 1 (3.3) | |
| Galicia | 2 (6.7) | |
| La Rioja | 1 (3.3) | |
| Madrid | 9 (30) | |
| Murcia | 1 (3.3) | |
| Basque Country | 1 (3.3) | |
| Valencia | 1 (3.3) | |
| Age | 30–50 years | 18 (60) |
| >50 years | 12 (40) | |
| Years of experience in caring for PLWH | <5 years | 7 (23.3) |
| 5–10 years | 1 (3.3) | |
| >10 years | 22 (73.3) | |
| How many PLWH do you attend in a month? | <100 | 4 (13.3) |
| 100–300 | 18 (60) | |
| >300 | 8 (26.7) | |
| What would you say is your level of familiarity with the CMO methodology? | Low | 11 (36.7) |
| Medium | 15 (50) | |
| High | 4 (13.3) | |
| What would you say is your level of knowledge with the CMO methodology? | Low | 12 (40) |
| Medium | 14 (46.7) | |
| High | 4 (13.3) | |
| Your level of knowledge regarding the available publications on the application of the methodology is: | Low | 14 (46.7) |
| Medium | 11 (36.7) | |
| High | 5 (16.7) | |
| How important do you believe it is to apply Pharmaceutical Care according to the CMO methodology today? | Low | 3 (10) |
| Moderate | 9 (30) | |
| High | 18 (60) | |
| How do you believe the implementation of Pharmaceutical Care according to the CMO methodology could improve the quality of life for patients today? | Low | 2 (6.7) |
| Moderate | 10 (33.3) | |
| High | 18 (60) | |
| How do you believe the implementation of Pharmaceutical Care according to the CMO methodology could improve health outcomes for patients today? | Low | 1 (3.3) |
| Moderate | 8 (26.7) | |
| High | 21 (70) | |
| How important do you consider patient stratification at both the medical and pharmaceutical levels today | Low | 0 |
| Medium | 3 (10) | |
| High | 27 (90) | |
| How important do you consider motivational interviewing in consultations (both at the medical and pharmaceutical levels) today? | Low | 0 |
| Medium | 4 (13.3) | |
| High | 26 (86.7) | |
| How important do you consider remote patient monitoring (telemedicine-telepharmacy) today? | Low | 0 |
| Medium | 8 (26.7) | |
| High | 22 (73.3) | |
| Is the CMO methodology applied in practice in daily patient care at your center, either fully or partially? | No | 13 (43.3) |
| Yes | 5 (16.7) | |
| I don't know | 12 (40) | |
| In the case of having any practical experience in applying the CMO methodology at your center, what is your level of satisfaction? (N = 19) | Low | 0 |
| Moderate | 8 (42.1) | |
| High | 11(57.9) | |
| Would you be willing to or encourage your pharmaceutical colleagues to implement the CMO methodology at your center (in case it is not currently applied)? | Low | 1 (3.3) |
| Moderate | 9 (30) | |
| High | 20 (66.7) | |
| Do you believe it would bring any benefits at the medical level? | No | 0 |
| Yes | 30 (100) | |
| I don't know | 0 | |
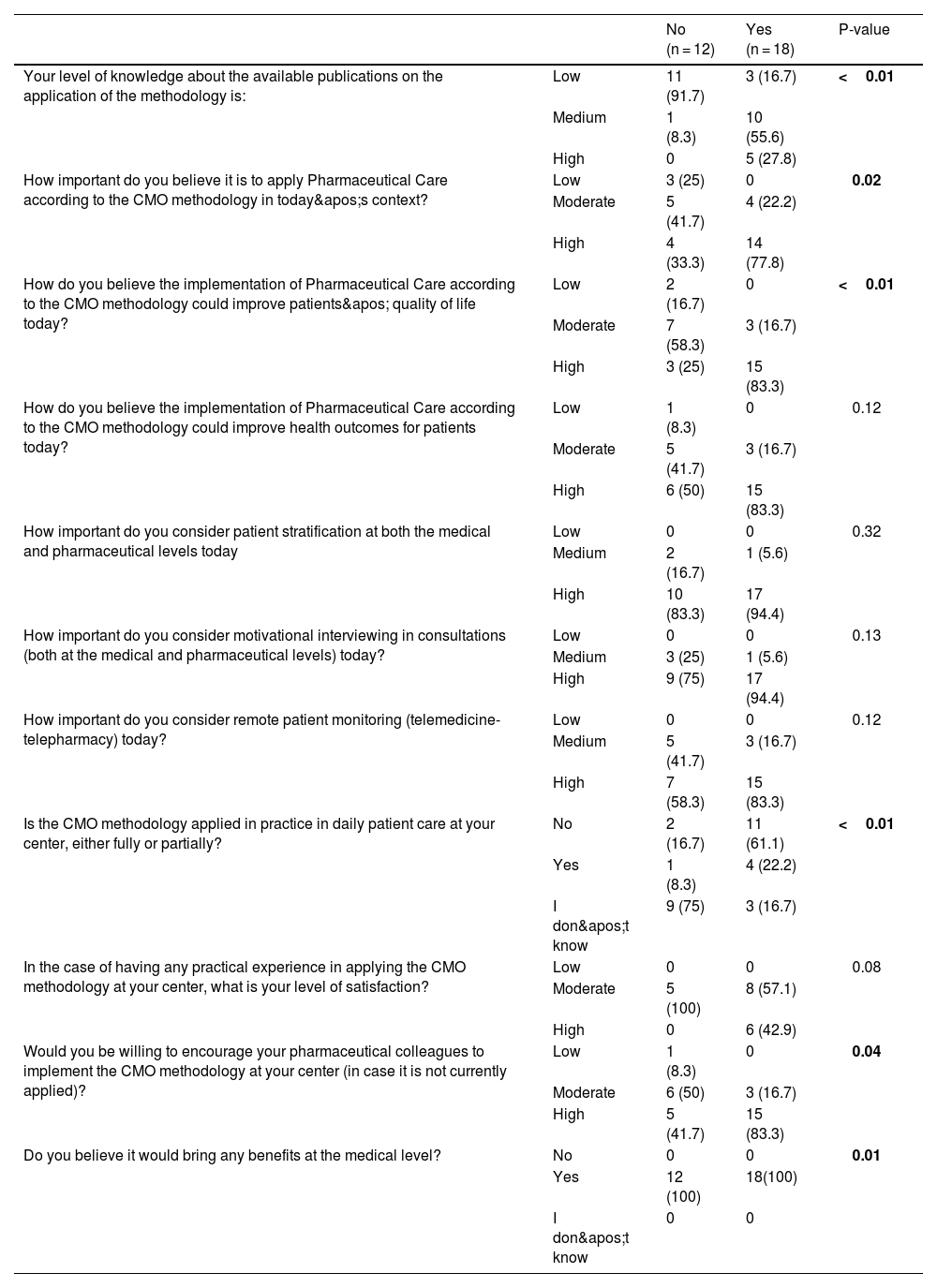
Knowledge of the CMO methodology was moderate-to-high in 60% of participants. This group demonstrated statistically significant differences in their perception of the importance of implementing PC based on this methodology compared to those with low knowledge (p = 0.02). Furthermore, participants with greater knowledge believed that implementing the methodology could improve both quality of life (p < 0.01) and health outcomes (p = 0.12). Table 2 provides the complete results of the bivariate analysis.
Results of the Bivariate Analysis Based on Knowledge of the CMO Methodology.
| No (n = 12) | Yes (n = 18) | P-value | ||
|---|---|---|---|---|
| Your level of knowledge about the available publications on the application of the methodology is: | Low | 11 (91.7) | 3 (16.7) | <0.01 |
| Medium | 1 (8.3) | 10 (55.6) | ||
| High | 0 | 5 (27.8) | ||
| How important do you believe it is to apply Pharmaceutical Care according to the CMO methodology in today's context? | Low | 3 (25) | 0 | 0.02 |
| Moderate | 5 (41.7) | 4 (22.2) | ||
| High | 4 (33.3) | 14 (77.8) | ||
| How do you believe the implementation of Pharmaceutical Care according to the CMO methodology could improve patients' quality of life today? | Low | 2 (16.7) | 0 | <0.01 |
| Moderate | 7 (58.3) | 3 (16.7) | ||
| High | 3 (25) | 15 (83.3) | ||
| How do you believe the implementation of Pharmaceutical Care according to the CMO methodology could improve health outcomes for patients today? | Low | 1 (8.3) | 0 | 0.12 |
| Moderate | 5 (41.7) | 3 (16.7) | ||
| High | 6 (50) | 15 (83.3) | ||
| How important do you consider patient stratification at both the medical and pharmaceutical levels today | Low | 0 | 0 | 0.32 |
| Medium | 2 (16.7) | 1 (5.6) | ||
| High | 10 (83.3) | 17 (94.4) | ||
| How important do you consider motivational interviewing in consultations (both at the medical and pharmaceutical levels) today? | Low | 0 | 0 | 0.13 |
| Medium | 3 (25) | 1 (5.6) | ||
| High | 9 (75) | 17 (94.4) | ||
| How important do you consider remote patient monitoring (telemedicine-telepharmacy) today? | Low | 0 | 0 | 0.12 |
| Medium | 5 (41.7) | 3 (16.7) | ||
| High | 7 (58.3) | 15 (83.3) | ||
| Is the CMO methodology applied in practice in daily patient care at your center, either fully or partially? | No | 2 (16.7) | 11 (61.1) | <0.01 |
| Yes | 1 (8.3) | 4 (22.2) | ||
| I don't know | 9 (75) | 3 (16.7) | ||
| In the case of having any practical experience in applying the CMO methodology at your center, what is your level of satisfaction? | Low | 0 | 0 | 0.08 |
| Moderate | 5 (100) | 8 (57.1) | ||
| High | 0 | 6 (42.9) | ||
| Would you be willing to encourage your pharmaceutical colleagues to implement the CMO methodology at your center (in case it is not currently applied)? | Low | 1 (8.3) | 0 | 0.04 |
| Moderate | 6 (50) | 3 (16.7) | ||
| High | 5 (41.7) | 15 (83.3) | ||
| Do you believe it would bring any benefits at the medical level? | No | 0 | 0 | 0.01 |
| Yes | 12 (100) | 18(100) | ||
| I don't know | 0 | 0 |
Regarding the different pillars of the CMO model, 90% of respondents considered stratification to be of high importance. Additionally, 86.7% rated motivational interviewing as highly beneficial, with greater appreciation observed among participants with more advanced knowledge of the methodology. Remote monitoring of PLWH via telemedicine and/or telepharmacy was deemed highly relevant by 73.3% of respondents.
DiscussionThis study demonstrates that the CMO methodology is positively valued by medical specialists, although general knowledge about it remains limited.
The level of knowledge about the CMO model is directly associated with a greater perception of its clinical relevance and an increased willingness to implement it. This finding aligns with the principle of lifelong learning, widely recognized as fundamental for ensuring professional competence and optimizing pharmacotherapeutic and healthcare outcomes in dynamic healthcare settings.10,11 These results are consistent with previous studies highlighting the integration of innovative models that can significantly improve inter-level care quality and therapeutic outcomes.12,13
However, the findings also reveal considerable heterogeneity in the adoption of the model. Despite the recognition of fundamental pillars and tools such as care stratification as critical for improving health outcomes, their practical application remains nascent and insufficient.14,15
Integrating pharmacists into care teams emerges as a key strategy to ensure the effective implementation of the CMO model. Successful experiences have shown how active pharmacist participation contributes to optimizing multidisciplinary management, improving treatment adherence, and increasing patient satisfaction.6 This level of multidisciplinary collaboration is essential for addressing the complex needs of PLWH and achieving a positive impact on patient health outcomes.
A crucial strategy for overcoming the observed variability could involve the development of training programs for both physicians and pharmacists, focusing on the practical benefits of the CMO model, particularly in key areas such as stratification, motivational interviewing, and telehealth. Additionally, pilot initiatives integrating this methodology into specific contexts could facilitate its progressive adoption.
This study has several limitations, including its cross-sectional design and the use of a self-administered questionnaire. Nevertheless, the study design accounted for these circumstances, and the methodology aimed to ensure sample representativeness and minimize potential biases associated with the self-selective nature of participation. Employing complementary methodologies, such as semi-structured interviews or focus groups, could enhance understanding of the barriers and facilitators to adopting this model. Future research should focus on longitudinal designs and evaluating the impact of specific interventions aimed at promoting model implementation.
In conclusion, the CMO model represents an innovative opportunity to transform PC. The widespread implementation of this model, supported by national educational strategies, the integration of information technologies, and the promotion of standardized practices, has the potential to improve health outcomes and care quality. This approach can consolidate a patient-centered, excellence-oriented care paradigm aligned with the strategic objectives of the MAPEX project.
Declaration of authorshipThe corresponding author, on behalf of all authors, certifies that:
- 1.
Each of the persons indicated as authors has made a direct and significant contribution to the intellectual content of the work.
- 2.
All authors have reviewed and approved the contents of the manuscript submitted to the editorial process.
- 3.
Each of them has given their consent for their name to appear in the authorship of the manuscript.
Enrique Contreras Macías: Writing – review & editing, Writing – original draft, Visualization, Validation, Investigation, Formal analysis, Data curation. Pilar Taberner Bonastre: Writing – review & editing, Visualization, Validation, Methodology, Investigation. Anaïs Corma Gómez: Writing – review & editing, Visualization, Validation, Methodology. José Ramón Blanco Ramos: Writing – original draft, Visualization, Validation, Supervision, Investigation, Conceptualization. Ramón Morillo Verdugo: Writing – review & editing, Visualization, Validation, Supervision, Investigation, Conceptualization.
Ethical considerationsThe study protocol and any other relevant documentation were reviewed and approved by the Research Ethics Committee of Sevilla Sur (code SICEIA-2024-000342).
FundingThe authors declare that they have not received any funding for the development of the study.
The authors declare that they have no conflicts of interest.

