



The objective of this study was to assess the results of applying Lean Methodology in the design of a standardized medication storage model in hospitalization departments.
MethodDescriptive and retrospective study conducted between September 2017 and January 2019 in a tertiary level hospital. The Pharmacy Service led the creation of a multidisciplinary team. Lean Methodology was used to establish the components and organization and identification criteria that made up the standardized medication storage model. The stocks of each hospitalization department were reviewed and quantified, the final amount of stock needed was agreed with the supervisor of each department, and the economic impact of the implementation of the standardized medication model was assessed. A questionnaire was designed and sent to nursing staff to determine their level of satisfaction with the new model.
ResultsThe standardized medication storage model was scaled up to 20 nursing departments, leading to an overall reduction of 56.72% in the number of pharmaceutical dosage forms available (5,688 vs 2,462). The number of high-risk drugs was reduced by 40.73% (631 vs 374). This elimination of wastage achieved a saving of €25,357.98. A total of 58 nurses returned the questionnaires (20.70% of the total): 22.40% worked a fixed shift and 77.60% worked a rotating shift. The mean score on overall satisfaction was 5.79 ± 3.61 (scores ranged from 1 to 10).
ConclusionsThe application of Lean Methodology is very useful for the management of medication stocks in hospitalization departments. The implementation of a standardized medication storage model leads to economic savings and a marked reduction in the number of active ingredients and high-risk medications. The nursing staff were satisfied with the implementation of the model, suggesting that we should continue to pursue this effective line of action.
El objetivo del estudio es evaluar los resultados de la aplicación de la metodología Lean en el diseño de un modelo estandarizado de almacenaje de medicación en las unidades de hospitalización.
MétodoEstudio descriptivo y retrospectivo desarrollado entre septiembre de 2017 y enero de 2019 en un hospital de tercer nivel. Se creó un equipo multidisciplinar liderado por el Servicio de Farmacia. Se empleó la metodología Lean para establecer los elementos y criterios de organización e identificación que conformaron el modelo estandarizado de almacenaje de medicación. Se revisaron y cuantificaron los stocks de cada unidad de hospitalización, se consensuó la medicación con la supervisora de cada unidad y se estimó el impacto económico de la implantación del modelo estandarizado. Se diseñó y envió una encuesta para evaluar la satisfacción de enfermería con el nuevo modelo.
ResultadosEl modelo estandarizado de almacenaje se aplicó en 20 unidades de enfermería y supuso una reducción global del 56,72% en el número de presentaciones de principios activos disponibles (5.688 versus 2.462). Se disminuyó el número de presentaciones de principios activos de medicamentos de alto riesgo en un 40,73% (631 versus 374). La eliminación de este despilfarro supuso un ahorro económico de 25.357,98 €. Se recibieron 58 respuestas a la encuesta de satisfacción del personal de enfermería (20,70% del total de encuestas enviadas), de las que un 22,40% correspondieron al turno fijo y 77,60% al turno rotativo. La media de la satisfacción global (valorada entre 1 y 10) fue de 5,79 ± 3,61.
ConclusionesLa aplicación de la metodología Lean es útil para la gestión de stocks de medicación de las unidades de hospitalización. La implantación del modelo estandarizado de almacenaje conlleva un ahorro económico y una reducción del número de presentaciones de principios activos y de medicamentos de alto riesgo. El personal de enfermería está conforme con la implantación del modelo, lo que nos plantea seguir en esta línea de mejora.
The Quality Plan Strategy of the Spanish National Health System includes the improvement of patient safety in health centres as a priority, with a special focus on the need to implement quality systems1.
In order to improve quality and safety, many health care systems have adopted solutions such as Lean Management, which was initially created within the industrial sector2. This methodology includes a set of practices or tools whose objective is to improve the workplace by identifying opportunities for improvement. These practices include the assessment of current processes in order to reduce “waste”, create value, and increase quality3. This methodology has come to maturity in the automotive and logistics sectors. Its adaptation to hospitals and the health care sector has become known as Lean Management in Healthcare4. This approach includes several tools that can be applied to the hospital health care context such as 5S, visual control, standardisation, priority matrix, and value chain analysis. Its implementation has led to rapid improvements adapted to real needs and has a marked impact on staff, patients, and process management5,6. The 5S method was created in Japan and is based on five Japanese words that begin with S: Seiri (Sort), Seiton (Set in order), Seiso (Shine), Seiketsu (Standardize), and Shitsuke (Sustain). Its objective is to create and maintain an organized, clean, and safe workplace in which high-level processes can be conducted. Thus, 5S is considered to be a key factor in the implementation of Lean Management7.
Regarding dispensing medication in hospitals, the Unit Dose Distribution System provides patients with the highest level of safety. This method involves the daily dispensing of individualized medication8. However, all nursing departments have medication kits for emergency access to medications. These kits should be adapted to include the drugs most widely used in the department. The drugs should be rationally organised, stored in previously agreed fixed amounts, and correctly labelled. High-risk drugs (HRD) and dangerous drugs should also be easily differentiated from all other drugs9,10. Final responsibility for the management of medication kits rests on the hospital pharmacy11, although other health care and management bodies are also involved.
After the implementation of innovations aimed at improving safety in health systems12, it is advisable to assess the level of satisfaction of the health care staff involved. The assessment process should include nursing staff subgroups to take into account different types of shifts and different work departments13. Although Lean Techniques have been widely used in the health care sector, little is known regarding their effectiveness or on levels of satisfaction among health care staff after their implementation14–17.
The main objective of this study was to assess the results of applying Lean Methodology in the design of a standardized storage model in the hospitalization departments (HD) of a tertiary university hospital and assess the level of satisfaction among health care staff after its implantation. Secondary objectives were to describe the design, pilot, and scaling stages of the model's implementation.
MethodsDescriptive and retrospective study conducted between September 2017 and January 2019 in a 1,200-bed tertiary university hospital.
A multidisciplinary team was created comprising five pharmacists, two quality and innovation staff, and two preventive medicine staff. Two external experts (a doctor and a nurse) working in the area of clinical and health care acted as consultants. The study also received the support of the hospital's medical and nursing management. Periodic meetings were scheduled.
The Lean Healthcare tools used were process and components standardization, priority matrix, visual control, value chain analysis, and the wastage of medication stock.
Design and pilot stageWe conducted a 5S analysis of the HD medication storage models and identified opportunities to improve efficiency.
We designed a standardized medication storage model and established organization and identification criteria. A systematic workflow was established to optimize the amount of medication needed in each HD. This was conducted in three stages:
- 1
Initial inventory: the quality assurance nurses quantified the drugs available in the HD stock, recording them on an Excel spreadsheet. The pharmacist assigned costs to the drugs and identified the HRDs.
- 2
Medication agreement: a consensus was reached between the pharmacist, nursing supervisor, and head of the HD service on the final amount of medication stock needed. Consensus was based on medication turnover during the last six months in each department. The newly agreed stock level was compared with the initial inventory and the excess drugs were withdrawn. These drugs were considered to lack added value and were viewed as wastage.
- 3
Implementation: after reaching agreement on drug stock, the supervisor of each HD withdrew the excess medication and the quality assurance nurses reorganized the stock by identifying and labelling the boxes in a standardized way according to the model criteria. To finalize this stage and complete the process, the pharmacist adapted the open lists of electronic stock-based requests for medication in each HD to the new agreement.
After completing the design and work flow, a pilot run was conducted in the internal medicine department.
Scaling-up stageNext, the working group created a schedule for implementing the process in all the HDs, with meetings every two months for assessment and follow-up.
The measurement variables were the number and cost of the initial and final drug units (i.e. to determine wastage), the number of pharmaceutical dosage forms per each active ingredient, and HRDs in stock before and after the implementation of the Lean Model.
Assessment stageThe Nursing Management team sent the nursing staff of the departments involved a secure internal email message containing the link to the questionnaires. The user satisfaction questionnaire was designed to assess whether the new storage model increased perceived safety and facilitated the management of medications in the department, especially HRDs (Figure 1). The questionnaire collected information on the type of schedule of the nursing staff (fixed or rotating shifts) and the department in which they worked (the nursing staff were subsequently classified into surgical or medical departments). The questionnaire comprised six closed questions using a Likert-type response scale. Three of the questions were scored from 1 to 5, where 1 represented the lowest value and 5 represented the highest. These items referred to safety when accessing medication, ease of access to medication and the visual organization of the medication boxes. The three remaining questions had a yes/no format and referred to whether the identification of the medication by active ingredient was correct, whether staff knew the meaning of the round red stickers placed on the boxes, and whether the probability of medication errors was reduced with the measures implemented.

We calculated an overall satisfaction score, which ranged between 1 and 10.
A statistical analysis was conducted using the SPSS version 19 software package to determine if there was an association between the six questionnaire items (i.e. “ease of access to medication”, “safety when accessing medication”, “visual organization of storage”, “correct identification by active ingredient”, “knowledge of the meaning of the round red stickers”, and “decrease in medication errors”) and the nursing staff's type of shift schedule and/or the type of nursing department. The score of the responses to the first three items was divided into two categories: scores of 1 and 2 were considered negative and scores of 3, 4, and 5 were considered positive.
Regarding overall satisfaction, we analysed the normality of the data distribution in each group and applied the Mann-Whitney U test to compare the values between the groups, ascertain any differences, and determine their significance.
A P-value of <.05 was used as a cutoff for statistical significance.
ResultsDesign and pilot stageThe following opportunities for improvement were identified in relation to the medication stock in the HD: variations in the type of medication container, variations in the organization and identification criteria applied to the medication boxes, absence of standardized labels to facilitate access to correct medication, and the accumulation of unnecessary medication with consequent waste and economic costs.
The multidisciplinary team established a standardized model for the medication storage in the HD based on the following criteria:
- 1
Structural components that made up the model: a commercial wall cabinet with two or three arrays of boxes depending on the requirements of the department's medication kit; a drawer trolley under the worktop for medications that did not fit into the boxes; and a poster to raise awareness about HRDs (the poster was put up on the left side of the wall).
- 2
Organization of the medication: medication was organised according to the route of administration with oral and parenteral medications being stored separately. Oral medications were stored in the upper area of the wall cabinet, intravenous medications below them, and finally subcutaneous medications. Likewise, active ingredients were stored in alphabetical order and from lower to higher dose, starting in the upper left corner and ending in the lower right corner.
- 3
Identification of the medication: a 12-mm Dymo device was used to create labels with black capital letters on a white background for oral medications and black capital letters on a blue background for parenteral medications. The label with the name of the active ingredient was placed in the upper centre of the box. In those cases in which the active ingredient did not unambiguously identify the drug, a larger label with the commercial name was placed in the lower right corner of the box.
HRDs were identified by placing a round red circular label in the middle of the boxes.
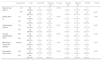
Scaling-up stageThe standardized model was scaled up to 20 nursing departments, achieving an overall saving of €25,357.98, which represented 56.04% of the initial costs (see Table 1). The number of different pharmaceutical dosage forms per active ingredient was reduced from 5,688 in the initial stock to 2,462 in the final stock (i.e. 3,226 units; 56.72%). The number of HRDs in the medication kits was reduced from 631 in the initial stock to 374 in the final stock (i.e. 257 units; 40.73%).
Results of the implementation of a standardized medication storage model in hospitalization departments
| Nursing Department | Clinical Service | € lnitial | € Final | Wast1 | N° lnitial Al | N° Final Al | N° Wasted Al | N° lnitial Al HRD | N° Final Al HRD | N° Wasted Al HRD |
|---|---|---|---|---|---|---|---|---|---|---|
| EA01 | Gastroenterology | 2,752.22 € | 786.86 € | 1,965.36 € (71.41%) | 321 | 109 | 212 (66.04 %) | 31 | 16 | 15 (48.39%) |
| EA02 | Traumatology | 2,028.94 € | 446.66 € | 1,582.28 € (77.99%) | 195 | 115 | 80 (41.03%) | 24 | 23 | 1 (4.17%) |
| EA03 | Oncology | 3,708.54 € | 871.72 € | 2,836.82 € (76.49%) | 326 | 148 | 178 (54.60%) | 20 | 0 | 20 (100.00%) |
| EA04 | Cardiology (intermediate) | 1,105.29 € | 468.13 € | 637.16 € (57.65%) | 311 | 142 | 169 (54.34%) | 37 | 29 | 8 (21.62%) |
| EB01 | Gastrointestinal and General Surgery | 2,335.33 € | 1,147.53 € | 1,187.80 € (50.86%) | 393 | 122 | 271 (68.96%) | 43 | 23 | 20 (46.51%) |
| EB02 | Traumatology and Plastic Surgery | 1,362.65 € | 446.66 € | 915.99 € (67.22%) | 209 | 115 | 94 (44.98%) | 19 | 23 | −4 (−21.05%) |
| EB03 | Haematology and Haemotherapy | 3,230.74 € | 1,499.67 € | 1,731.07 € (53.58%) | 244 | 134 | 110 (45.08%) | 28 | 18 | 10 (35.71%) |
| EB04 | Cardiology | 3,077.56 € | 1,193.60 € | 1,883.96 € (61.22%) | 449 | 145 | 304 (67.71%) | 49 | 27 | 22 (44.90%) |
| EC01 | General Surgery | 3,206.31€ | 607.24 € | 2,599.07 € (81.06%) | 241 | 91 | 150 (62.24%) | 40 | 23 | 17 (42.50%) |
| EC02 | Pulmonology | 1,680.32 € | 1,000.06 € | 680.26 € (40.48%) | 239 | 134 | 105 (63.93%) | 31 | 21 | 10 (32.26%) |
| EC03 | Interna! Medicine | 2,687.30 € | 531.69 € | 2,155.61€ (80.21%) | 323 | 133 | 190 (58.82%) | 39 | 24 | 15 (38.46%) |
| EC04 | Thoracic Surgery and Vascular Surgery | 2,517.57 € | 1,138.26 € | 1,379.31€ (54.79%) | 300 | 165 | 135 (45.00%) | 33 | 22 | 11 (33.33%) |
| ED01 | Urology and Otorhinolaryngology | 770.05 € | 451.24 € | 318.81€ (41.40%) | 208 | 80 | 128 (61.54%) | 17 | 10 | 7 (41.18%) |
| ED02 | Neurology | 2,711.56 € | 2,530.32 € | 181.24 € (6.68%) | 237 | 96 | 141 (59.49%) | 43 | 18 | 25 (58.14%) |
| ED03 | Internal Medicine | 2,921.22 € | 1,106.02 € | 1,815.20 € (62.14%) | 416 | 144 | 272 (65.38%) | 36 | 24 | 12 (33.33%) |
| ED04 | Gynaecology and Maternity | 1,951.79 € | 1,574.43 € | 377.36 € (19.33%) | 278 | 150 | 128 (46.04%) | 27 | 19 | 8 (29.63%) |
| EE01 | Psychiatry | 2,200.33 € | 1,718.52 € | 481.81€ (21.90%) | 237 | 117 | 120 (50.63%) | 21 | 9 | 12 (57.14%) |
| EE02 | Short Stay and Neurology Unit | 1,969.85 € | 477.85 € | 1,492.00 € (75.74%) | 325 | 97 | 228 (70.15%) | 42 | 15 | 27 (64.29%) |
| EF01 | Psychiatry | 1,683.70 € | 1,238.45 € | 445.25 € (26.44%) | 237 | 117 | 120 (50.63%) | 21 | 9 | 12 (57.14%) |
| EF02 | Neurosurgery and Nephrology | 1,349.24 € | 657.62 € | 691.62 € (51.26%) | 199 | 108 | 91 (45.73%) | 30 | 21 | 9 (30.00%) |
| 45,250.51 € | 19,892.53 € | 25,357.98 € (56,04%) | 5,688 | 2,462 | 3,226 (56,72%) | 631 | 374 | 257 (40.73%) |
AI: active ingredient; HRD: high-risk drug.
Waste1: defined according to LEAN methodology. Understood as something that does not provide added value in this part of the process or area.
Source: Data collection registry of the inventory record of the Modelo Corporativo de Almacenaje de Medicación en las Unidades Planta (“Centre Model of Medication Storage in Hospital Departments”). Hospital Álvaro Cunqueiro MCAMUP Project. EOXI Vigo, 2019.
Of the 280 questionnaires, 185 were sent to nurses from medical departments. A total of 58 nurses (20.70%) filled in and returned the questionnaires: 22.40% worked a fixed shift, 77.60% worked a rotating shift, and 25.8% did not specify the department to which they belonged. Table 2 shows the results of the questionnaire by the frequencies and percentages of the items in each of the groups. No statistically significant association (P < .05) was found between the six items assessed in the questionnaire and the type of shift (fixed or rotating) or the type of department (surgical or medical).
Results of the satisfaction survey on the new medication storage model by type of shift and nursing department
| Assessment | Total | Fixed shift | Rotating shift | P value | Surgical ND | Medical ND | DK/NR | P value | |
|---|---|---|---|---|---|---|---|---|---|
| Ease of use (item 1) |
| 20 (34.5%) | 2 (10.0%) | 18 (90.0%) | 0.184 | 1 (5.0%) | 14 (70.0%) | 5 (25.0%) | |
| 38 (65.5%) | 11 (28.9%) | 27 (71.1%) | 6 (15.8%) | 22 (57.9%) | 10 (26.3%) | 0.391 | |||
| Safety (item 2) | 1-2 | 11 (19.0%) | 1 (9.1%) | 10 (90.9%) | 0.426 | 1 (9.1%) | 9 (81.8%) | 1 (9.1%) | 1.000 |
| 3-5 | 47 (81.0%) | 12 (25.5%) | 35 (74.5%) | 6 (12.8%) | 27 (57.4%) | 14 (29.8%) | |||
| Visual layout (item 3) | 1-2 | 24 (41.4%) | 2 (8.3%) | 22 (91.7%) | 0.031 | 2 (8.3%) | 18 (75.0%) | 4 (16.7%) | 0.420 |
| 3-5 | 34 (58.6%) | 11 (32.4%) | 23 (67.6%) | 5 (14.7%) | 18 (52.9%) | 11 (32.4%) | |||
| Correct identification of AI | Yes | 46 (79.3%) | 12 (26.1%) | 34 (73.9%) | 0.264 | 5 (10.9%) | 27 (58.7%) | 14 (30.4%) | 1.000 |
| No | 12 (20.7%) | 1 (8.3%) | 11 (91.7%) | 2 (16.7%) | 9 (75.0%) | 1 (8.3%) | |||
| Meaning of round red stickers | Yes No | 35 (60.3%) | 10 (28.6%) | 25 (71.4%) | 0.165 | 4 (11.4%) | 28 (80.0%) | 3 (8.6%) | 0.347 |
| 23 (39.7%) | 3 (13.0%) | 20 (87.0%) | 3 (13.0%) | 8 (34.8%) | 12 (52.2%) | ||||
| Decreased risk of error | Yes | 37 (64.9%) | 10 (27.0%) | 27 (73.0%) | 0.346 | 6 (16.2%) | 20 (54.0%) | 11 (29.8%) | 0.222 |
| No | 20 (35.1%) | 3 (15.0%) | 17 (85.0%) | 1 (5.0%) | 15 (75.0%) | 4 (20.0%) |
AI: active ingredient; DK: don't know; ND: nursing department; NR: no reply.
Figure 2 shows “overall satisfaction” by score, which ranged between 1 and 10. The mean score was 5.79 ± 3.61. Regarding the implementation of the storage model, 69.40% of the nurses reported a level of satisfaction of more than 5. The mean levels of satisfaction in the fixed-shift group and the rotating-shift group were 6.69 ± 2.25 and 5.20 ± 2.36 (P = .031), respectively. No statistically significant differences were found between the type of department (surgical or medical) (6.00 ± 2.82 and 5.22 ± 2.43, respectively; P = .429).
Discussion
Standardization is needed to deliver higher quality health care. The application of various Lean methodology tools to an area of drug management (i.e. the medication kits in the HD) facilitated the design and implementation of a standardized medication storage model.
D'Andreamatteo et al.18 suggested that projects based on Lean Methodology represent a strategic choice for entire organizations and must led by the management team. Our Lean Methodology-based project was presented to the Management Committee and was supported by both the Medical and Nursing Management. Therefore, we agree with the vision of D'Andreamatteo et al. that entire health organizations need to commit to the implementation of these types of projects.
One of the Lean Tools used, 5S methodology was of particular relevance in our study. In fact, 5S tools have also been used in previous studies that have implemented Lean Methodology to improve health care, such as the one conducted by Sari et al.19. These authors studied the level of economic investment in the implementation of Lean initiatives to improve quality and health in health care. They estimated that, over the period 2012 to 2014, the total cost of implementing a Lean Approach, including consultants and new hires, ranged between $44 million CAD to $49.6 million CAD. They suggested that the outcomes of these investments should be assessed prior to Lean implementation. In our study, the application of the Lean methodology led to quite different economic costs for the following reasons: it was conducted without external consultants; the multidisciplinary expert team were already part of the staff; and the team included staff from the Hospital's Quality Assurance department. Thus, the only real cost, which was negligible, was purchasing the identification labels and printing the HRD posters
Fields et al.20 addressed the use of Lean methodologies to streamline the processing of requests for medical equipment and supplies for children with complex conditions. They estimated that the decrease in processing time led to annual cost savings of approximately $11,000. Their study, like ours, quantified economic “waste” after the implementation of Lean methodology, although it differed from ours in the scope of its implementation.
Our successful attempt to reduce the number of HRDs in the HD medication kits was in line with the recommendations of the Collaboration Agreement between the Ministry of Health and Consumer Affairs and the University of Salamanca. This agreement addresses activities related to improving the safe use of medicines in Spanish hospitals and establishes that the number of dosage forms of HRDs in the Pharmacotherapeutic Guide or in a specific health care department should be reduced to a minimum in order to reduce the risk of error10.
Previous studies have applied Lean Methodology in several areas of hospital pharmacy: sterile products areas14, the categorisation of the activities of clinical pharmacists as “waste” or “non-waste”15, pharmacy residency training programs16, and the analysis of the factors affecting medication safety in mental health facilities17. However, the literature search did not find any study related to the application of Lean methodology to drug management in medication kits at hospitals.
Our study opens up a new line of research strategy, in the sense that it has pioneered the quantification of waste in medication storage in HDs. Although it is clearly relevant to use Lean methodology to improve quality, we must do this in practical terms by quantifying the waste costs determined by the use of Lean. In this study we achieved savings of €25,357.98 in medication stock.
In total, 69.40% of the nurses reported being satisfied (≥ 5 points) with the implementation of the new storage model. This percentage was higher than that found in the study by Berdot et al.21 in which 56% of nurses were satisfied with traditional storage. However, their objective differed from ours in that their study compared automated drug dispensing cabinets versus traditional storage.
In our study, the survey response rate was 20.70%. Although low, other studies, such as that of Parekh et al.22, have reported rates as low as 12.6%. However, their study differed from ours because it compared doctors and nurses and because their survey had a different rationale. On the other hand, other studies, such as that conducted by Ardern-Jones et al.23, have reported response rates as high as 77.9%, due to the fact that the questionnaires was re-distributed two weeks after the initial distribution. Their study had fewer participants, included physicians, and assessed the implementation of an automated storage system.
Regarding type of department, 66% of the questionnaires were sent to nurses from medical departments. This percentage is similar to that reported by other studies. The returned questionnaires showed that 62% of the nurses belonged to this type of department.
This study is limited by the low number of staff who responded to the survey and the high percentage of respondents who did not specify the type of department in which they worked.
The standardized medication storage model identified significant waste (56%) through the intradepartmental pharmacy medication agreement in the HDs.
Most of the staff who responded to the survey on the standardized storage model considered that the implemented measures had increased safety.
In conclusion, we planned, implemented, and assessed a set of measures over a 16-month period involving Medical and Nursing management, middle managers, the Pharmacy Service, and the Quality and Innovation department. This initiative had a real and marked impact on improving effectiveness and efficiency in optimizing the process, patient and staff safety, and quality of care.
FundingNo funding.
AcknowledgmentsWe would to extend our thanks to all the EOXI Vigo staff who collaborated in the development of this project. We would also like to thank the Methodology and Statistics Unit of IIS Galicia Sur for all the help provided.
Conflict of interestNo conflict of interests.
Presentation at congressesPart of this work has been presented as an oral communication at the 21st National Congress of Hospitals and Health Management, Santiago de Compostela, Spain (May 8, 2019).
Part of this work was included within the project entitled: “Improvement in drug safety: impact of a global strategy for prevention and risk management”. It received a Special Prize from the Jury in the IV Convocatoria del Premio Sham (2019).
Contribution to the scientific literature
This study presents the application of several Lean-methodology tools to medication kits in hospitalization departments.
It also provides data on the level of satisfaction of health care staff with the outcomes of using this methodology to improve the safety of the medication storage process.
Grupo de Trabajo de Almacenaje de Medicación de la EOXI Vigo:
Hadriana Fernández-Vega. Fundación biomédica de Pontevedra, Vigo y Orense (Servicio Gallego de Salud, SERGAS), Vigo. Spain.
Belén Leboreiro-Enríquez. Servicio de Farmacia, Xerencia de Xestión Integrada de Vigo (Servicio Gallego de Salud, SERGAS), Vigo. Spain.
Susana San Martín-Álvarez. Servicio de Farmacia, Xerencia de Xestión Integrada de Vigo (Servicio Gallego de Salud, SERGAS), Vigo. Spain.
Carmen Gallastegui-Otero. Servicio de Farmacia, Xerencia de Xestión Integrada de Vigo (Servicio Gallego de Salud, SERGAS), Vigo. Spain.
Antonio Pérez-Landeiro. Servicio de Farmacia, Xerencia de Xestión Integrada de Vigo (Servicio Gallego de Salud, SERGAS), Vigo. Spain.
Cristina Casanova-Martínez. Fundación biomédica de Pontevedra, Vigo y Orense (Servicio Gallego de Salud, SERGAS), Vigo. Spain.
Karina Lorenzo-Lorenzo. Servicio de Farmacia, Xerencia de Xestión Integrada de Vigo (Servicio Gallego de Salud, SERGAS), Vigo. Spain.
Alicia Martín-Vila. Servicio de Farmacia. Centro Sanitario Centro Penitenciario A Lama, Pontevedra. Spain.
Inmaculada Pardo-Lemos. Unidad de Calidad e Innovación, Xerencia de Xestión Integrada de Vigo (Servicio Gallego de Salud, SERGAS), Vigo. Spain.
Esther Casal-Rodríguez. Dirección Médica, Xerencia de Xestión Integrada de Vigo (SERGAS), Vigo. Spain.
María Dolores Muíños-Pérez. Subdirección de Enfermería, Xerencia de Xestión Integrada de Vigo (SERGAS), Vigo. Spain.
Susana Cerqueiro-Gómez. Dirección Médica, Xerencia de Xestión Integrada de Vigo (SERGAS), Vigo. Spain.

