
To study medication adherence and persistence among heart failure patients, assess the methods utilised for estimating medication adherence, and identify optimal adherence thresholds and their impact on clinical outcomes.
MethodsA systematic search will be conducted in PubMed, Embase, CINAHL, Web of Science, and Scopus databases. Observational studies assessing medication adherence or persistence among heart failure patients via electronic healthcare databases will be included. A narrative synthesis will describe medication adherence and persistence reported and methods used to measure it. A meta-analysis will be attempted to evaluate the impact of secondary medication adherence (multiple and by drug class) on clinical outcomes, including hospitalisation, emergency visits, and mortality. The I2 statistic will be employed to study heterogeneity and the GRADE framework to evaluate evidence certainty. This protocol follows the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols guidelines and is registered with the Prospective Register of Ongoing Systematic Reviews CRD42024509542.
DiscussionThis study aims to evaluate medication adherence and persistence in heart failure management through electronic health databases, intending to explore widely used measurement methods and their limitations, and to identify adherence thresholds associated with improved clinical outcomes. By examining these aspects, we anticipate proposing enhancements for future research and establishing desired adherence goals. This approach highlights the expected significance of our findings in advancing patient care and research methodologies.
Estudiar la adherencia y persistencia a la medicación en pacientes con insuficiencia cardíaca, evaluar los métodos utilizados para estimar la adherencia a la medicación, e identificar umbrales de adherencia óptimos y su impacto en los resultados clínicos.
MétodosSe realizará una búsqueda sistemática en las bases de datos PubMed, Embase, CINAHL, Web of Science y Scopus. Se incluirán estudios observacionales que evalúen la adherencia o persistencia de la medicación en pacientes con insuficiencia cardíaca a través de bases de datos sanitarias electrónicas. Se describirá la adherencia y persistencia recogida en los estudios y la metodología empleada para ello mediante síntesis narrativa. Si es factible, se realizará un metaanálisis para evaluar el impacto de la adherencia secundaria a la medicación (múltiple y por grupo terapéutico) en resultados clínicos, incluyendo hospitalización, episodios de urgencias y mortalidad. Se emplearán el estadístico I2 para estudiar la heterogeneidad y el marco GRADE para evaluar la certeza de la evidencia. Este protocolo sigue las recomendaciones de las guías PRISMA-P (Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols) y está registrado en PROSPERO (Prospective Register of Ongoing Systematic Reviews) CRD42024509542.
DiscusiónEste estudio tiene como objetivo dilucidar las complejidades que rodean el cumplimiento del tratamiento en pacientes con insuficiencia cardíaca. Determinar el nivel actual de adherencia a la medicación y los umbrales óptimos nos permitirá definir la situación actual y los objetivos de adherencia necesarios para mejorar los resultados clínicos. Además, comprender las limitaciones de los métodos de medición de adherencia actuales guiará futuras mejoras en la investigación. Se espera que los hallazgos contribuyan a mejorar la atención al paciente mediante la implementación de estrategias específicas de mejora de la adherencia y perfeccionar las metodologías de investigación en este campo.
Enhancing therapeutic outcomes in heart failure (HF)—reducing hospitalisations, decreasing cardiovascular mortality, and improving disease management— through medical treatments, requires adherence to prescribed medication regimens. While the precise threshold of adherence needed to optimise treatment response in HF patients remains undefined,1 it is documented that non-adherence rates vary between 20% and 50%,2,3 with significant associations with poor health outcomes, including increased mortality and hospital readmissions.4–6 Evidence strongly suggests that enhancing adherence can significantly reduce these risks.7–9 This underscores the critical need for accurately characterising patient medication adherence and implementing targeted interventions to improve it.
Multiple approaches have been established to quantify medication adherence, with the utilisation of prescription records for indirect adherence assessment gaining prominence through improved access to electronic health records and administrative data.10,11 Accurately assessing medication adherence in broad populations through comprehensive administrative data requires records from all prescribed medications and their refill histories.12 These data are highly relevant for determining medication effectiveness, identifying factors associated with poor adherence, and implementing interventions to improve it.13 Therefore, adherence evaluations through these databases can provide insights into real-world patients' use of HF medications, providing valuable information for clinical practice.
To our knowledge, efforts to systematically evaluate and synthesise evidence on medication adherence in patients with HF have been limited. Furthermore, there is a significant gap in research concerning identifying optimal adherence thresholds and exploring their impact on clinical outcomes. Hence, this systematic review aims to examine the existing literature to: Firstly, to investigate medication adherence and persistence among patients with HF and evaluate the methods used for estimating medication adherence via electronic healthcare databases; and secondly, to identify optimal adherence thresholds for this population and examine their association with clinical outcomes.
MethodsStudy design overviewThis systematic review and meta-analysis are designed to answer the PICOS question: (Population), patients with HF; (Intervention), HF pharmacological management; (Comparator) Not applicable; (Outcome): Medication adherence and persistence measured using electronic health databases; (Study design), observational studies.
This protocol has been recorded in the Prospective Register of Ongoing Systematic Reviews under the registration CRD42024509542, and it adheres to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis Protocols guidelines (PRISMA-P 2015).14
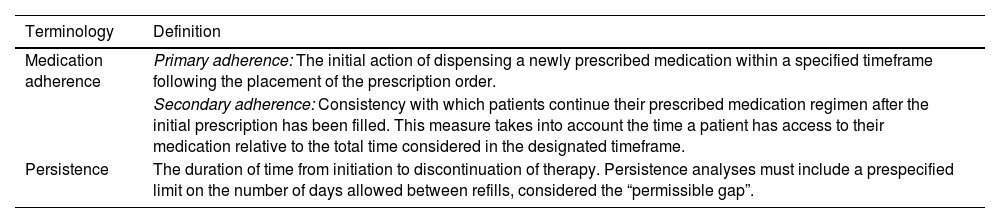
Medication adherence is defined as the degree to which patients use their medications as prescribed by their healthcare providers.15 This principle can be divided in primary and secondary adherence and is complemented by persistence. Table 1 collects the definitions of these concepts which will be utilised for this review.
Medication adherence definitions.
| Terminology | Definition |
|---|---|
| Medication adherence | Primary adherence: The initial action of dispensing a newly prescribed medication within a specified timeframe following the placement of the prescription order. |
| Secondary adherence: Consistency with which patients continue their prescribed medication regimen after the initial prescription has been filled. This measure takes into account the time a patient has access to their medication relative to the total time considered in the designated timeframe. | |
| Persistence | The duration of time from initiation to discontinuation of therapy. Persistence analyses must include a prespecified limit on the number of days allowed between refills, considered the “permissible gap”. |
Adapted from Raebel et al.19
For definitions of electronic healthcare databases and a list of medications considered for HF management, please consult supplementary material 1 and table S1, respectively.
Eligibility criteriaTo be included, studies must comply with all inclusion criteria and none of the exclusion criteria.
Inclusion criteria- •
Population: HF patients. The study will include only those populations consisting solely of patients diagnosed with HF.
- •
Measurements: At least one estimate of adherence or persistence (See Table 1) must be carried out for medications considered for HF management (See supplementary material table S1) utilising electronic healthcare databases as data sources.
- •
Study type: Observational studies.
- •
Publication period: Studies published from 1990 to 2024.
- •
Studies focusing on adherence to non-pharmacological interventions, including advice on physical activity, fluid or sodium consumption, and dietary guidelines, as well as studies assessing adherence to clinical guidelines.
- •
Studies which used adherence measures relying on methods such as pill counts, self-reports, assessments by providers or caregivers, or electronic monitoring devices.
- •
Evaluations that utilised data from patient's registries or disease management programs exclusively.
- •
Investigations where data were obtained through the manual transcription or review of information from an automated system.
- •
Research that necessitated the manual examination of medical records to gather data.
- •
Research involving fewer than 100 patients.
- •
Analyses restricted to the use of medications in an inpatient setting.
- •
Publications in the form of poster abstracts, editorials, reviews, or commentaries.
- •
Studies written in languages other than English, French, Italian, or Spanish.
The search for studies will be conducted in the following electronic databases: Medical Literature Analysis and Retrieval System Online (MEDLINE) through PubMed, EMBASE, CINAHL, Scopus, and Web of Science. Abstracts and full texts will be sourced for every article deemed suitable for inclusion.
The search will employ Medical Subject Headings or their equivalents, along with keywords and free-text terms. The search approach will be customised for the previously mentioned databases. Detailed search strategies for all databases explored can be found in the supplementary material table S2.
Furthermore, the reference lists of all included articles will be manually reviewed, and a citation analysis will be performed to identify additional studies potentially missed by the initial search. Following the conclusion of the final analysis, and prior to the drafting of the final manuscript the search will be updated to include recent publications, which will then be evaluated for inclusion in the review.
Study screening and selectionIndependently and concurrently 2 reviewers will conduct the article selection process. Following the removal of duplicate entries, an initial screening will be performed based on titles and abstracts, with a comprehensive review involving full-text reading as necessary. Any differences in article selection will be settled through consensus or decided by a third reviewer. The rationale for excluding any studies will be documented.
Data collectionSelected articles will be assessed, and relevant information will be systematically collected and recorded in a structured database using Microsoft Excel, Microsoft Corporation (Redmond, WA, USA). Data to be extracted will include: study design, study population characteristics, settings, study dates and duration, aims, adherence and persistence rates, methods and related parameters used for assessing medication adherence or persistence, and clinical outcomes evaluated. If the same cohort is reported twice or more, the data will be extracted from the most recent study or the one with the largest sample.
Data synthesisThe first step will involve conducting a narrative synthesis to aggregate and summarise findings from the identified studies. This will be followed by an attempt to perform a meta-analysis focused on studies investigating the relationship between medication adherence and clinical outcomes. This analysis will depend upon the data's suitability, specifically the availability and heterogeneity of the studies in question.
Narrative synthesisIn this study, estimates of medication adherence in HF patients, as well as adherence measures used will be sought. Accordingly, adherence and persistence measures estimated using various healthcare databases will be the focus of this narrative synthesis, and study findings will be grouped by type (i.e., primary adherence, secondary adherence, persistence), definition/equation, and determination of cut-off values or thresholds for medication adherence measures.
Meta-analysisA meta-analysis will examine the association between medication secondary adherence (multiple and by drug class), and clinical outcomes, including but not restricted to hospitalisations, emergency visits, and mortality. The impact of dichotomised adherence thresholds will be assessed. Odds ratios (OR), along with 95% confidence intervals will be calculated to express the associations between adherence and outcomes. The OR and its standard error will be transformed into natural logarithms. This will be done to stabilise the variance and normalise their distributions. Heterogeneity will be evaluated using the I2 test. Pooled effect sizes and their 95% confidence intervals will be determined by a random effects model. The analysis will be conducted using RevMan 5.4.1, with results presented in forest plots and funnel plots to assess publication bias.
Assessment of study quality and bias riskTwo reviewers will evaluate the included studies for risk of bias and quality of reporting. In cases of disagreement, a third reviewer will be consulted for resolution. The Joanna Briggs Institute checklist will be utilised to assess the risk of bias.16 A narrative summary will present the outcomes of the bias risk assessments, with detailed evaluations available in an appendix. The TEN-SPIDERS tool will be used to evaluate the reporting of the methodologies used to measure secondary medication adherence.17
Additionally, the confidence in the evidence from studies included in the meta-analysis will be determined using the Grading of Recommendations, Assessment, Development, and Evaluations framework.18
DiscussionStrengths and limitationsTo our knowledge, this will be the first systematic review and meta-analysis to compile medication adherence and persistence measures in HF patients using healthcare databases.
Our study's strengths include applying a thorough systematic review methodology featuring clear, reproducible eligibility criteria, and comprehensive search strategies for study screening and data extraction. Screening will be independently conducted in pairs by trained reviewers, ensuring reliability. Furthermore, using data from electronic health databases allows large populations to be included, so the results obtained can be representative of the study population.
However, the study faces limitations due to its reliance on retrospective data, such as biases from missing information and the inability of claims databases to verify medication intake or capture inpatient medication usage, directly impacting the accuracy and comprehensiveness of adherence measures.
Implications of this studyThe results of this study will provide a detailed overview of the most commonly employed methods for utilising electronic healthcare databases as data sources in measuring adherence. It will also delineate their limitations, and pinpoint effective adherence thresholds associated with enhanced clinical outcomes in this population.
By highlighting these methods' limitations, we aim to propose enhancements for future research to address these issues. Identifying the ideal adherence threshold will recognise the desired adherence objective for our patients. This approach highlights the practical significance of our findings in enhancing patient care and refining research methodologies.
Funding sourcesThe authors received no specific funding for this work.
Ethical considerationsThe authors declare no ethical considerations.
CRediT authorship contribution statementNerea Baéz-Gutiérrez: Writing – review & editing, Writing – original draft, Visualization, Validation, Methodology, Conceptualization. Héctor Rodríguez-Ramallo: Writing – review & editing, Writing – original draft, Visualization, Validation, Supervision, Methodology, Conceptualization. Susana Sánchez-Fidalgo: Validation, Supervision.
Supplementary file 1

