






Verify the importance of compliance by prescribed doses of high-alert medications in unit of pediatric emergency in patient safety.
MethodThis was a cross-sectional descriptive study conducted in a unit of pediatric emergency, for March to April of 2012. This study included all prescriptions that contained at least one high-alert medication, excluding all of others. The data were analyzed using Microsoft Office Excel® version 2007, and the study was approved by the Research Ethics Committee of the Hospital.
ResultsThis study included prescriptions for 100 patients with a mean age of 5.2 ± 4.2 years. Were identified 983 (40.1%) high-alert medications (21 different), with predominance of injectable solutions (834, 84,8%), and of these 727 (73.95%) were electrolytes. The analysis of the dose was possible for 641 electrolytes and 104 non-electrolytes, being the dose inadequacies observed for some medications. Was observed concentration absent to 189 (18.9%) prescribed medications, these with liquid pharmaceutical form or aerosol. Was observed also the absence of maximum dose for 8 (36.3%) prescribed drugs “if necessary”.
ConclusiónThe inadequacies of doses of high-alert medications identified in this study may compromise patient safety, demonstrating the importance of knowledge of multidisciplinary health care team by this subject, in this context, it is noteworthy that the acting of a clinical pharmacist together with the health multidisciplined team can contributes with the review of drug prescriptions, reducing potential errors and collaborating with patient safety.
Investigar la importancia de la conformidad de las dosis prescritas de los medicamentos potencialmente peligrosos en un hospital pediátrico de urgencia en la garantía de la seguridad del paciente.
MétodoEstudio descriptivo transversal realizado en una unidad de atención de urgencia pediátrica, referente a los meses de marzo y abril de 2012. Se incluyeron todas las prescripciones que contienen al menos un medicamento potencialmente peligroso, excluyendo todas las otras. Los datos fueron analizados utilizando Microsoft Office Excel® versión 2007, y el estudio fue aprobado por el Comité Ético de Investigación Institucional.
ResultadosSe incluyeron prescripciones de 100 pacientes con 5,2 ± 4,2 años de edad. Se identificaron 983 (40,1%) medicamentos potencialmente peligrosos (21 diferentes), con mayoría de la soluciones inyectables (834, 84,8%), siendo 727 (73,95%) electrolitos. El análisis de las dosis fue posible para 641 medicamentos electrolitos y 104 no electrolitos, observándose non conformidad de dosis para algunos medicamentos. Fue posible constatar que la concentración de los fármacos estuvo ausente para 189 (18,9%) medicamentos prescritos con forma farmacéutica líquida y/o aerosoles. También se observó la ausencia de las dosis máximas de 8 (36,3%) medicamentos prescritos “si es necesario”.
ConclusiónLas non conformidad en las dosis de medicamentos potencialmente peligrosos identificados en el presente estudio pueden comprometer la seguridad del paciente, lo que demuestra la importancia del equipo multidisciplinario de atención a la salud tener conocimiento de este tema. En este contexto, cabe destacar que la actuación de un farmacéutico clínico insertado en este equipo puede contribuir para la revisión de las prescripciones de medicamentos, lo que reduce los posibles errores y colabora con la seguridad del paciente.
High-alert medications are drugs that have a high risk of causing significant adverse events to patients when used erroneously.1 The Institute for Safe Medication Practices (ISMP) defines and annually updates a list of all the medicines classified as high-alert, with special focus on agonists and adrenergic antagonists, antiarrhythmics, anti-thrombotic drugs, opioids, sedatives, concentrated electrolytes, among others.2
It is known that about 58% of the harm caused by medications in hospitals is attributed to high-alert medi-cations.3 Although such errors are not the most common, when they do occur they tend to be of high severity and can result in prolonged hospitalization, cause permanent injury, and even prove fatal.4
During hospitalization, the profile of the population being treated is one of the factors that may contribute to a higher incidence of medication errors.5 For example, certain characteristics of the pediatric population can be associated with the highest incidence of medication errors in this patient group, including: 1) calculation of doses based on body weight; 2) frequent use of off-label medications; 3) hepatic and renal immaturity; 4) accidental self-administration of medications.6
Another factor considered high risk for the occurrence of medication errors is services characterized by a high patient turnover rate, particularly urgent and emergency services.5
Amongst the errors that can occur in the use of medicines, prescription errors are the most serious.7 Thus, special care should be taken to avoid errors in prescriptions for pediatric patients in use of high-alert medications, more specifically those involving dosing of prescribed drugs. There is little difference in therapeutical concentrations and toxicity of most high-alert medications,1 highlighting the need for careful monitoring of doses, clinical effects, as well as of the sera levels of high-alert medications among patients in use of these drugs.4
High quality prescription of medicines is essential in the hospital setting, since this constitutes the first step toward preventing medication errors and increasing patient safety.8
In a preliminary evaluation of the quality of prescriptions to pediatric patients in the Emergency Service involved in this study, a high incidence of errors was detected along with high consumption of high-alert medications (21.4%).9 This situation, compounded by the absence of a clinical pharmacist available at the study venue, prompted the current investigation. In this context, the aim of the present study was to verify the importance of conformity of the prescribed doses of high-alert medications within a hospital pediatric emergency unit in the safeguarding of patient safety.
MethodsA descriptive, cross-sectional study was conducted in the Pediatric Emergency Department (SERUPE) of a university hospital in the Mid-western region of Brazil between 01 March and 30 April 2012. The institution in which the study was carried out is a tertiary level hospital that provides healthcare exclusively to users of the public health system. The unit has 12 hospital beds and provides care to patients aged 0 to 16 years in urgent and emergency situations.
The study included all prescriptions for patients seen at the SERUPE in the period analyzed, which contained at least one prescribed high-alert medication, excluding all other prescriptions. Data collection was performed using a structured form developed for this study. The form was previously validated by data collection of the prescriptions of the unit, evaluated for seven days. The structured form comprises two parts: 1) general data on patient (age, gender, weight, type of intervention); and 2) general data on medicines (drug, dose, concentration, dosage, route of administration).
The subjects were classified into five age groups: newborns (0-28 days), infants (29 days to less than 2 years), preschool children (2 years to under 7 years), school children (7 years to under 10 years) and adolescents (over 10 years).10
For the weight variable, the presence of this information in the patient’s medical record was checked. With respect to the type of intervention performed, subjects were classified according to type of intervention into physician or surgical, with surgical patients considered those submitted to an invasive procedure during the hospital stay.
The identified medicines were classified by therapeutic sub-group according to level 2 of Anatomical Therapeutic Chemical (ATC) classification.11
The evaluation parameters of dosage errors related to high-alert medications were: concentration, overdose/ underdose, absence of maximum dose for prescribed drugs “if necessary” and dose omission.
The identification of concentration of prescribed drugs applied only to liquid and aerosol pharmaceutical forms, being oral or injectable, since the other medicines analyzed were solid pharmaceutical forms.
The therapeutic range of high-alert medication was determined according to the Blackbook® fourth edition,12 as depicted in table 1. The Holliday-Seger method was used to analyze the adequacy of electrolyte doses prescribed for maintenance of hydroelectrolytic balance.13 In this study, the term “electrolyte” is used to refer to three electrolytes: dextrose 50%, sodium chloride (NaCl) 20%, and potassium chloride (KCl) 10% injectables. These reference values were adopted because they are widely used in the healthcare unit under study.
Therapeutic range considered for the analysis of medications non-electrolytes prescribed in the Service of Pediatric Urgency in the period from 01 March to 30 April 2012, according to the fourth edition of Pediatrics Blackbook
| Drugs | Doses recommended | ||
|---|---|---|---|
| Minimum | Maximum | Daily Maximum | |
| Codeine + Acetaminophen3 | 1 mg/kg | - | 2 to 6 years = 30 mg Over 6 years = 60 mg |
| Digoxin4 | 10 µg/kg | 40 µg/kg | -** |
| Dobutamine12 µg/kg/min | 40 µg/kg/min | -** | |
| Enoxaparine11 mg/kg | 3 mg/kg | -** | |
| Epinephrine1 | 0,1 mg/kg | 5 mg/kg | -** |
| Fentanyl1 | 0,5 µg/kg/hour | 5 µg/kg/hour | -** |
| Ketamine1 | 2 mg/kg | 60 mg/kg | -** |
| Magnesium sulfate 50%1 | 0,2 mEq/kg ou 25 mg/kg/dose | - | 2g/dose (4-6 daily doses) |
| Midazolam1 | 0,05 mg/kg | 25,92 mg/kg | 10 mg |
| Morphine1 | 0,15 mg/kg | 144 mg/kg/dia | *** |
| Non-fractioned heparin1 | 50 U/kg | 100 U/kg | -** |
| NPH insulin1 | * | * | -** |
| Potassium chloride 6%2 | 1 mEq/kg | 5 mEq/kg | -** |
| Promethazine10,4 mg/kg | 6 mg/kg | -** | |
| Propranolol3 | 0,5 mg/kg | 8 mg/kg | Arrhythmia = 60 mg Hypertension = 640 |
| Regular insulin1 | * | * | -** |
| Salbutamol5 | 100 µg/dose | 800 µg/dose | -** |
| Tramadol1 | 4 mg/kg/day | 12 mg/kg/day | 400 |
1Injectable solution; 2Syrup; 3Tablet; 4Elixir; 5Aerosol.
*The dose varies by capillary blood glucose test; ** Don’t have maximum daily dose established on the reference consulted; *** Don’t have maximum dose established on the reference consulted. Doses must be titrated and adjusted according to clinical response from the recommended starting dose.
Electrolytes prescribed in the absence of the following information: dose, infusion rate, patient weight and/or hydroelectrolytic maintenance indication, were excluded from the analysis of dose adequacy. This omission is justified by the requirement of this information in order to use the Holliday-Seger method. In relation to electrolytes, those lacking concentration information, in the case of pharmaceutical liquid and aerosol forms, and those without weight data, were excluded from the dose adequacy analysis because the prescribed dose could not be calculated.
Data were keyed into and analyzed using Microsoft Office Excel®, 2007 version. This study was submitted to the Research Ethics Committee of the hospital and approved under protocol number 078/2011, and conforms to the ethical principles of Brazilian Resolution 196/96 and supplementary rules of the National Health Council.14 The requirement for written informed consent was waived because the study only entailed a search of medical records.
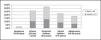
ResultsDuring the study period, a total of 450 prescriptions from 110 patients were identified, however, 69 prescriptions were excluded because they did not contain highalert medication (7.7%) or omitted information on patient weight (7.5%). Therefore, the study included a final total of 381 (84.6%) prescriptions containing 2451 drugs, of which 983 (40.1%) were high-alert medications. The prescriptions were derived from 100 (90.9%) patients (mean of 3.8 and median of 3 prescriptions/ patient) with a mean age of 5.2 ± 4.2 years, ranging from 15 days to 14 years old. Figure 1 depicts the profile of patients prescribed high-alert medication by age and gender.

Information regarding patients’ weight was present in 92 (92.0%) records. Regarding the reason for consultations, 95 (95.0%) patients sought care for clinical treatment, 03 (3.0%) for surgical treatment, and the remainder (2.0%) for removal of foreign bodies or for reasons not reported in medical records at the time of data collection.
The analysis identified 21 different high-alert medications prescribed, as shown in table 2, which were classified according to therapeutic class based on the ATC classfication11 (Table 3).
High-alert medication prescribed in the Pediatric Emergency Service in the period from March 01 to April 30-2012
| Drugs | Drugs prescribed | Drugs with prescribed dose | ||
|---|---|---|---|---|
| (n = 983) | (%) | (n = 836) | (%) | |
| Codeine + Acetaminophen3 | 15 | 1,5 | 15 | 100,0 |
| Dextrose 50%1 | 34 | 3,5 | 33 | 97,0 |
| Digoxin4 | 6 | 0,6 | 0 | 0,0 |
| Dobutamine1 | 2 | 0,2 | 1 | 50,0 |
| Enoxaparine1 | 3 | 0,3 | 3 | 100,0 |
| Epinephrine1 | 11 | 1,1 | 0 | 0,0 |
| Fentanyl1 | 13 | 1,3 | 11 | 84,6 |
| Ketamine1 | 2 | 0,2 | 1 | 50,0 |
| Magnesium sulfate 50%1 | 1 | 0,1 | 1 | 100,0 |
| Midazolam1 | 16 | 1,6 | 13 | 81,2 |
| Morphine1 | 23 | 2,3 | 23 | 100,0 |
| Non-fractioned heparin1 | 4 | 0,4 | 4 | 100,0 |
| NPH insulin1 | 4 | 0,4 | 2 | 50,0 |
| Potassium chloride 10%1 | 346 | 35,2 | 345 | 99,7 |
| Potassium chloride 6%2 | 1 | 0,1 | 1 | 100,0 |
| Promethazine1 | 6 | 0,6 | 0 | 0,0 |
| Propranolol3 | 2 | 0,2 | 2 | 100,0 |
| Regular insulin1 | 6 | 0,6 | 2 | 33,3 |
| Salbutamol5 | 120 | 12,2 | 8 | 6,6 |
| Sodium chloride 20%1 | 347 | 35,3 | 346 | 99,7 |
| Tramadol1 | 21 | 2,1 | 21 | 100,0 |
1 Injectable solution; 2 Syrup; 3 Tablet; 4 Elixir; 5 Aerosol.
Classification according to the Anatomical Therapeutic Chemical (ATC) of high-alert medication prescribed in the Pediatric Emergency Service in the period from March 01 to April 30-2012
| ATC Classification | High-alert medications | Number of high-alert medication by therapeutic class |
|---|---|---|
| Anti-thrombotic agent | Enoxaparine1Non-fractioned heparin1 | 7 (0,7%) |
| Agent beta-blocker | Propranolol3 | 2 (0,2%) |
| Codeine + acetaminophen3 | ||
| Analgesic | Morphine1 Tramadol1 | 59 (6,0%) |
| Anesthetic | Ketamine1 | 15 (1,6%) |
| Fentanyl1 | ||
| Antihistaminic for systemic use | Promethazine1 | 6 (0,6%) |
| Cardiac therapy | Digoxin4 Dobutamine1 | 8 (0,8%) |
| Medications used in diabetes | NPH insulin1 | 10 (1,0%) |
| Regular insulin1 | ||
| Medications for obstructive diseases of the respiratory system | Salbutamol5 | 131 (13,3%) |
| Epinephrine1 | ||
| Mineral supplement | Potassium chloride 6%2 | 1 (0,1%) |
| Potassium chloride 10%1 | ||
| Plasma substitutes and perfusion solutions | Sodium chloride 20 %1 | 728 (74,1%) |
| Dextrose 50%1 Magnesium chloride 50%1 | ||
| Psychoepletic | Midazolam1 | 16 (1,6%) |
1 Injectable solution; 2 Syrup; 3 Tablet; 4 Elixir; 5 Aerosol.
On the assessment of the pharmaceutical form of prescriptions, there was a predominance of liquid and aerosol pharmaceutical forms (966, 98.3%), namely: 840 (85.0%) instances of injectable solutions, 120 (12.2%) aerosol and 6 (0.6%) elixir, while the others were oral solids (17, 1.7%). Analyzing the 966 prescriptions for liquid pharmaceutical and aerosol pharmaceutical forms, it was observed that 189 (18.9%) did not state the concentration of the drug prescribed, namely: in 100.0% of prescriptions for digoxin elixir, enoxaparin, unfractionated heparin, promethazine, tramadol and regular human insulin and NPH insulin, 93.3% for salbutamol in aerosol form; 90.9% for injectable adrenaline solution, and in 17 4% of prescriptions for morphine injectable solution.
Also, it was observed that 727 (73.95%) high-alert medications prescribed were for electrolytes. The therapeutic range was assessed for 641 of the prescriptions for electrolytes, which were: 28 (82.4%) for dextrose 50%, 306 (88.2%) for sodium chloride 20% and 307 (88.7%) for potassium chloride 10% (Figure 2). The remaining prescriptions of electrolytes were not evaluated for the following reasons: 83 failed to record patient weight while 03 had no dose prescribed, thus precluding analysis.

The analysis of adequacy of dose was possible for 104 of the 256 prescriptions for non-electrolyte medications. The others were not analyzed for the following reasons: 144 (56.2%) due to the absence of the dose prescribed, 4 (3.5%) prescriptions for unfractionated heparin owing to lack of information on patient weight; 2 (1.7%) for regular insulin prescriptions, and 2 (1 7%) for NPH insulin for not having the therapeutic range defined in the reference adopted, although these had been prescribed with stated dose. Prescribed doses for drugs other than electrolytes are given in table 4.
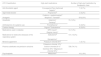
Prescribed dose of high-alert medication analyzed in Pediatric Emergency Service on period from March to April by 2012, according to the fourth edition of the Pediatrics Blackbook
| Drugs | Prescribed dose | ||
|---|---|---|---|
| Minimum | Maximum | ||
| Epinephrine1 | Without prescribed dose | ||
| Ketamine1 | 2,00 mg/kg | 2,00 mg/kg | |
| Potassium chloride 6%2 | 2,72 mEq/kg | 2,72 mEq/kg | |
| Codeine + Acetaminophen3 | 1,11 mg/kg | 3,92 mg/kg | |
| Digoxin4 | Without prescribed dose | ||
| Dobutamine1 | 0,01 µg/kg/min (continuous infusion) | 0,01 µg/kg/min | |
| Enoxaparine1 | 0,95 mg/kg | 0,95 mg/kg | |
| Fentanyl1 | 2,00 µg/kg/hour | 3,02 µg/kg/hour | |
| Non-fractioned heparin1 | Prescribed dose, but without the weight of patient | ||
| NPH insulin1 | * | * | |
| Regular insulin1 | * | * | |
| Midazolam1 | 0,63 mg/kg | 9,58 mg/kg | |
| Morphine1 | 0,21 mg/kg | 0,78 mg/kg | |
| Promethazine1 | Without prescribed dose | ||
| Propranolol3 | 1,11 mg/kg | 1,11 mg/kg | |
| Salbutamol5 | 100 µg/dose | 400 µg/dose | |
| Magnesium sulfate 50%1 | 0,65 mEq/kg or | 0,65 mEq/kg or | |
| 80 mg/kg | 80 mg/kg | ||
| Tramadol1 | 1,85 mg/kg/day (continuous infusion) | 14,91 mg/kg/day | |
1 Injectable solution; 2 Syrup; 3 Tablet; 4 Elixir; 5 Aerosol.
Note: The drugs that were used by Just one patient and had the same prescribed dose during the period of this study showed a minimum dose like to maximum dose.
Among the high-alert medications analyzed, 22 (2.2%) were prescribed “if necessary”, 14 (63.6%) of these corresponded to the therapeutic class of analgesics. There was also an absence of maximum dose information for 8 (36.3%) prescribed “if necessary” drugs, namely: adrenaline, ketamine, fentanyl, midazolam, morphine and tramadol in injectable solutions.
DiscussionThe percentage of high-alert medications observed in this study was far higher than figures reported by another study in Porto Alegre, Brazil, which found only 6.2% high-alert medications prescribed for a pediatric population of a tertiary level hospital.10 This relates to the fact that the unit assessed in the present study was an emergency service, which requires greater use of high-alert medications compared to an ordinary inpatient unit.
In this sense, it is noteworthy that the high-alert medications identified in this study are normally used in emergency services, highlighting the prevalence of the intravenous route of administration.15 Given this fact, the need for professionals qualified and accustomed with the use of injectable solutions requiring intravenous administration is evident, since their incorrect prescription or wrong administration can cause patients serious harm.16
The predominance of electrolytes among the drugs prescribed, mirroring findings in the literature,9 is explained by their wide use in maintenance therapy to help maintain the volume and composition of body fluids within normal ranges.17 The disparity observed between the prescribed doses and dosages recommended by the Holliday-Seger method may stem from the need to adjust the doses by increasing or decreasing the water and electrolytes for various clinical situations that modify normal losses of these.17
Errors related to electrolyte prescriptions for intravenous hydration have occurred frequently in the hospital setting, including fatal errors related to the administration of injectable potassium chloridee.18 It is known that administration of potassium chloride intravenously at excessively high speed, dose or concentration may result in cardiac arrest, and is reported as a cause of death worldwide.19 One study found that the main observed errors in prescriptions for potassium chloride 10% were related to the dose and pharmaceutical form.20
Another electrolyte which requires strict control in its use is sodium chloride 20%, since rapid changes in sodium concentration can result in serious complications such as cardiovascular shock, disorders of the central nervous system, hemolysis and kidney necrosis.19 Also concerning hydration maintenance therapy, it is important that patients using hypertonic dextrose are monitored closely for glucose levels, since hyperglycemia is associated to a worse prognosis, calling for adjustments in levels of glucose.21
The omission of dose information was an error that drew attention in this study. This fact, coupled with the characteristics of the drugs, possibly augments the risk related to care provided to patients. The presence of the dose of a drug in a prescription is indispensable, since it must be able to induce a pharmacological effect (efficacy) while presenting minimal toxicity (safety).22
The inadequacy of the recommended therapeutic range of doses of dobutamine, enoxaparin and tramadol was another important finding. The calculation of pediatric dose is a procedure that requires constant attention, since errors in calculations can cause adverse reactions and toxicity in overdose cases, or inefficacy in underdose cases.23
Specifically regarding enoxaparin, the underdosing in prescriptions may have been related to the non-availability of graduated syringes in Brazil, precluding the administration of the exact dose in some cases, for example in children. Thus, the prescriber may have chosen to use a subtherapeutic dose for this reason, or due to other unknown factors.
The tramadol maximum dose in mg/kg/day proved slightly higher than the recommended level. However, when observing the weight of patients with apparent overdoses, it was observed that the prescribed doses did not exceed the maximum recommended daily dose.
It is noteworthy, however, that the prescription dose is only one parameter related to patient safety, where other factors that are also important, such as dispensing, manipulation, administration, among others.2
The fact that data on patient body weight were absent in some records warrants special attention, since drug doses for pediatric patients are adjusted according to the child’s body weight or surface area.22 The absence of information on patient weight, as was observed for the medication unfractionated heparin, among others, can impair the correct calculation of the dose of the medicines to be prescribed. And where high-alert medication are involved, miscalculation can be fatal, since these have a lower margin of safety and are therefore more likely to harm the patients.2
It is also important, when considering pediatric patients, to know the physiological characteristics of the child and the pharmacokinetic parameters of the drug. The simple extrapolation of doses from adults to children, based only on body weight, body surface area or age, can have drastic consequences.22
The omission of the concentration of some medicines observed in this study is a flaw that may lead to the substitution of one pharmaceutical presentation for another. The absence of concentration is one of the most common errors observed,24,25 with rates of up to 22.1% for high-alert medications reported in the literature.24 Even where drug doses are prescribed, as was the case in this study, lack of concentration information can compromise patient safety in the process of dispensation and administration of drugs.
The predominance of analgesics prescribed as “if necessary” was similar to the finding of Santos and Heineck, although in their study, besides high-alert medication, off-label and unlicensed drugs were also evaluated.10 The absence of maximum dose for some drugs prescribed as “if necessary” is another problem impacting the safety of patients in use of high-alert medication observed in this study, since specification of minimum and maximum dose as well as the minimum interval between doses is necessary in prescriptions for these drugs.26
Lack of concordance among prescriptions for medicines is a significant indicator among medications errors and often these events go undetected, resulting in deficient therapy.24 In urgent and emergency units, most medication errors involve high-alert medications, since these are usually prescribed and administered without the review of a pharmacist,15 as was observed in the present study.
In Brazil, the multidisciplinary residency program proposes the involvement of the pharmacist in urgent and emergency care, underscoring the important role this professional has in ensuring patient safety in use of drugs and contributing toward assuring drug efficacy.25 The presence of pharmacists within clinical units is clearly associated with reductions in mortality and in adverse effects,27 however there are no studies in the area of emergency to demonstrate this fact.
The inclusion of clinical pharmacists in emergency services is mainly to perform a prospective review of prescriptions and to provide multidisciplinary teams with information on drugs, such as therapeutic dose adjustments according to kidney function, age, or weight; information availability and substitutability of drugs; recommendations on administration and any other guidance on the use of drugs or on restrictions.28
Some limitations were identified during the execution of this study, namely: lack of correlation between patient diagnosis and the prescribed doses of high-alert medication, a limiting factor in the accurate analysis of the therapeutic range; the impossibility of interventions when the occurrence of any inadequacies was noted, since this was a retrospective study; difficulty collecting and analyzing data due to the lack of institutional electronic medical records.
Despite the limitations identified, the findings highlight the need to review the processes of use of high-alert medication within the institution, especially: implementation of protocols for use; differentiated identification on packaging with warning about the proper use and segregated storage; deployment of double-checking procedures before prescription, dispensation and administration17; effective pharmacovigilance actions;29 inclusion of a clinical pharmacist on multidisciplinary teams; mandatory inclusion of patient weight in routine prescriptions, among others.
It is evident, therefore, that although the use of highalert medication in drug therapy is necessary within pediatric emergency units, this is a reality that poses numerous risks to the patient. It is in this context that the importance of the performance of a qualified health team emerges to ensure compliance of the prescribed doses of high-alert medication and of drug efficacy, where this represents only one of many aspects involved in patient safety.
Conflicts of interestThe authors have no conflict of interest to declare.

