
Chemotherapy-induced nausea and vomiting continue to pose a significant challenge for patients undergoing hematopoietic stem cell transplantation. This study aims to synthesize available evidence on antiemetic prophylaxis regimens in patients with hematologic malignancies undergoing hematopoietic stem cell transplantation, in order to identify the best standard of care.
MethodsA systematic review will be conducted using MEDLINE via PubMed, EMBASE, Clinical-Trials.gov., and Cochrane databases. Studies written in English, French, Italian, or Spanish will be considered. After screening the literature according to the inclusion and exclusion criteria, 2 independent reviewers will extract data and assess the risk of bias in eligible articles. This protocol has been prepared according to the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) guidelines. This protocol is registered in the Prospective Register of Ongoing Systematic Reviews (PROSPERO) CRD42023406380.
DiscussionChemotherapy-induced nausea and vomiting is a debilitating side effect that presents a significant challenge for patients with hematologic malignancies. Despite the publication of various guidelines, none of them include specific recommendations for each chemotherapy regimen. Therefore, analyzing the primary antiemetic prophylaxis regimens in patients with hematologic malignancies undergoing hematopoietic stem cell transplantation would be valuable in enhancing patients' quality of life.
Las náuseas y los vómitos inducidos por la quimioterapia siguen siendo un reto importante para los pacientes sometidos a trasplante de células madre hematopoyéticas. Este estudio tiene como objetivo sintetizar la evidencia disponible sobre los regímenes de profilaxis antiemética en pacientes con neoplasias hematológicas sometidos a trasplante de células madre hematopoyéticas, con el fin de identificar el mejor estándar de cuidado.
MétodosSe llevará a cabo una revisión sistemática utilizando las bases de datos MEDLINE a través de PubMed, EMBASE, Clinical-Trials.gov y Cochrane. Se considerarán los estudios escritos en inglés, francés, italiano o español. Después de seleccionar los estudios de acuerdo con los criterios de inclusión y exclusión, dos revisores independientes extraerán los datos y evaluarán el riesgo de sesgo en los artículos seleccionados. Este protocolo se ha elaborado de acuerdo con las recomendaciones de las guías PRISMA-P (Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols). Este protocolo está registrado en PROSPERO (Prospective Register of Ongoing Systematic Reviews) CRD42023406380.
DiscusiónLas náuseas y los vómitos inducidos por la quimioterapia son un efecto secundario incapacitante que supone un reto importante para los pacientes con neoplasias hematológicas. A pesar de la publicación de diversas guías sobre profilaxis antiemética, ninguna de ellas incluye recomendaciones específicas para cada régimen de quimioterapia. Por lo tanto, analizar los regímenes de profilaxis antiemética primaria en pacientes con neoplasias hematológicas sometidos a trasplante de progenitores hematopoyéticos sería valioso para mejorar la calidad de vida de estos pacientes.
Chemotherapy-induced nausea and vomiting (CINV) is a debilitating side effect that supposes a significant challenge for patients with hematologic malignancies. Not only can it persist for days or weeks after chemotherapy, but it can also negatively impact patient’s quality of life by causing electrolyte imbalances, dehydration, malnutrition, and weight loss1–3. Despite significant progress in understanding the physiological pathways and developing novel drugs to treat CINV, uncontrolled nausea and vomiting continue to affect 40–80% of chemotherapy patients1. Antiemetic prophylaxis in hematologic patients has been shown to prevent CINV in at least 70% of cases4,5.
CINV can be classified into acute and delayed phases, with the latter occurring between day 2 and day 5 after chemotherapy6. While there have been significant improvements in treating acute CINV with the development of 5-HT3 and NK-1 receptor antagonists, nausea and vomiting remains a significant clinical problem for patients receiving highly and moderately emetogenic chemotherapy (MEC and HEC, respectively) despite the use of proper pharmacologic prophylaxis7,8.
Patients with hematologic malignancies are particularly susceptible to delayed CINV as they often receive multiple first-line chemotherapy regimens, multi-day conditioning regimens, and salvage therapy. Healthcare professionals may also underestimate the incidence of delayed nausea and vomiting in these patients2,4.
The first proposal for monitoring CINV was published in 1997 and has been constantly updated by diverse oncologic societies, including the American Society of Clinical Oncology (ASCO)9, the Multinational Association of Supportive Care in Cancer (MASCC)10, the European Society for Medical Oncology (ESMO)11, and the National Comprehensive Cancer Network (NCCN)12. In 2017, the American Society of Clinical Oncology (ASCO) updated its guidelines, adding specific CINV prophylaxis for patients undergoing hematopoietic stem cell transplantation (HSCT), which should include a 3-drug combination of 5HT3-RA with dexamethasone and NK1-RA13. Still, none of the guidelines includes specific recommendations for each chemotherapy regimen4,14.
Based on the preceding, we will conduct a systematic review with the aim of comparing antiemetic prophylaxis regimens in hematologic malignancies patients undergoing a HSCT to identify the best standard of care, regarding efficacy, and safety.
MethodStudy design overviewThis systematic review was designed to answer the PICOS question: (Population), adult patients with hematological malignancy receiving highly emetogenic chemotherapy (HEC) or moderately emetogenic chemotherapy (MEC) within conditioning protocols for HSCT; (Intervention), antiemetic prophylaxis regimens, including neurokinin-1 (NK1) receptor antagonist, 5-hydroxytryptamine-3 (5-HT3) receptor antagonists, and/or corticosteroid and/or olanzapine;(Comparison) other antiemetic prophylaxis regimens; (Outcomes), complete control of vomiting and/or nausea during the overall phase, and adverse events; (Study design), Randomized clinical trials, systematic reviews, and meta-analysis.
This protocol is registered in the Prospective Register of Ongoing Systematic Reviews (PROSPERO) CRD42023406380 and was structured according to the Preferred Reporting Items for Systematic Review guidelines and Meta-Analysis Protocols (PRISMA-P 2015)15. The systematic review will be conducted according to PRISMA guidelines16.
Eligibility criteriaThe inclusion criteria are:
- -
Men and women ≥18 years of age with hematological malignancy receiving HEC or MEC within conditioning protocols for HSCT.
- -
Study design: Randomized clinical trials, systematic reviews, and meta-analysis
- -
Studies written in English, French, Italian, or Spanish will be considered.
- -
No time restrictions will be applied to this study.
The exclusion criteria are:
- -
Another etiology for emesis and nausea (e.g. gastrointestinal obstruction, increased intracranial pressure, hypercalcemia, and active peptic ulcer).
- -
Pregnant or nursing women.
- -
Other studies not indicated in the inclusion criteria (cohort studies, expert opinion, and narrative reviews).
The search for studies will be conducted in the following databases: Medical Literature Analysis and Retrieval System Online (MEDLINE) via PubMed, EMBASE (via Embase.com), Cochrane database, and Clinical-Trials.gov to include relevant trials in progress.
For each article selected for inclusion, abstracts and full articles will be obtained.
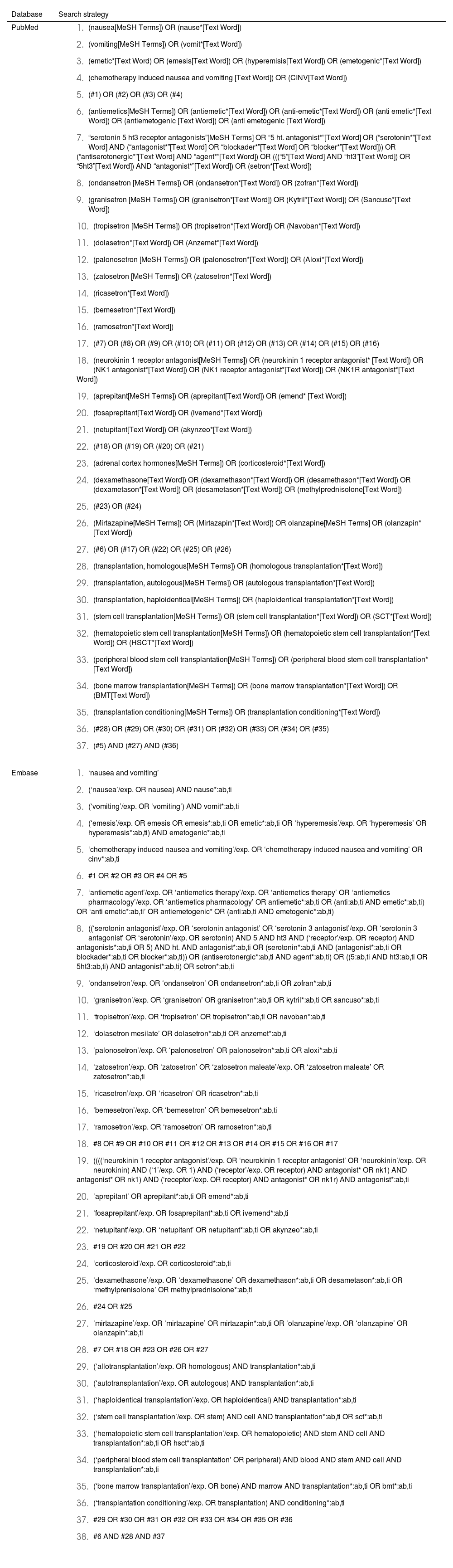
We will use Medical Subject Heading (MeSH) or equivalent, keywords, and free-text search terms. We will adapt the search strategy to the remaining databases previously mentioned. Table 1 lists the search strategies of the PubMed and Embase databases in detail.
Search strategy for the different databases.
| Database | Search strategy |
|---|---|
| PubMed |
|
| Embase |
|
The reference list of each article will be manually reviewed, and a citation analysis will be performed to identify articles missed by the search strategy.
The research will be repeated immediately after the final analysis in order to enable new studies to be revised. If the inclusion criteria are met, they can be included in this review.
Study screening and selectionThe selection of the articles will be carried out by 2 reviewers by duplicate and independently. After removing duplicates, a preliminary selection of papers will be made by analyzing titles and abstracts and the articles will be thoroughly examined by reading the entire text when required. The discrepancies in the selection will be resolved by consensus, and the decision will correspond to a third reviewer in the case of not reaching an agreement. The reasons for exclusion studies will be registered.
Data collectionFull-text copies of included articles will be reviewed, and data will be extracted and entered into a structured Microsoft Excel, Microsoft Corporation (Redmond, WA, USA) database. The following variables will be collected:
- •
Study characteristics: Study design, aims, setting and dates, and study duration.
- •
Patient characteristics: Average age or age limits for inclusion in each study, sex, ethnicity, number of participants recruited/allocated/evaluated, participants with lost to follow-up, hematological malignancy and stage, type of conditioning regimen (myeloablative, reduced-intensity, and non-myeloablative), number of days of chemotherapy, and emetogenic risk of the conditioning regimen.
- •
Outcomes measured: In this study, the primary outcome to be evaluated will be the complete control of nausea and vomiting in the acute, delayed, and overall phase.
Clinical trials' design to approve drugs for preventing and treating CINV and PONV has undergone changes to better evaluate the effectiveness of candidate products17. Initially, trials measured the proportion of patients with emetic episodes as the primary endpoint. As time progressed, trial endpoints expanded to include other factors, such as the use of rescue medication to assess Complete Response and the presence and severity of nausea in evaluating Complete Control, Total Response, and Total Control17. Although many tools have been used to assess nausea and vomiting, there is currently no standard outcome for clinical trials investigating the effects of interventions to control chemotherapy-induced nausea and vomiting in cancer patients18. Therefore, we will consider this a variable measurement instrument until we assess how the majority of studies included in this review are measured. In addition to nausea and vomiting, other variables investigated in the selected studies will also be identified.
The secondary outcomes of this study will include the incidence of adverse reactions, and the rate of improvement of quality of life.
Included studies will undergo a risk of bias and reporting quality assessment by 2 reviewers. If there is any disagreement, a third reviewer will be consulted. If there is still doubt regarding the methodology or the reporting of results, study authors will be contacted as appropriate. Included RCT will be assessed with the Cochrane Handbook's Risk of Bias (ROB) assessment tool19. The risk of bias assessment results will be summarized narratively, with complete assessments provided as an appendix.
Data synthesisA descriptive analysis of relevant study methodological and clinical characteristics will be provided. This summary will include the main study and patient features, interventions, reported outcomes, and risk of bias assessments.
DiscussionStrengths and limitationsTo the best of our knowledge, this is the first systematic review comparing antiemetic combination therapies to prevent chemotherapy-induced nausea and vomiting caused by HEC or MEC in hematological patients undergoing HSCT.
Our study has several strengths. First, we will utilize a rigorous systematic review methodology that includes explicit and reproducible eligibility criteria, as well as sensitive search strategies for both study screening and data extraction. Study screening will be conducted independently and in duplicate by teams of two trained reviewers.
However, our study also has some limitations. It will rely on reported trial information, and our findings may be vulnerable to underreporting or selective reporting20,21. Nonetheless, we will perform an exploratory search on clinicaltrials.gov to locate potential studies without reported results and minimize publication bias. Another limitation is that the study only includes articles published in English, French, Italian, and Spanish, which may result in the loss of relevant information written in other languages. Nevertheless, most published studies are expected to be available within these languages. Additionally, no restrictions will be imposed on the publication years of the selected studies.
Implications of this studyAs previously stated, the decision-making process for preventing CINV is often challenging for both patients and physicians due to the lack of specific recommendations for antiemetic agents in international guidelines in this context9,11. The findings of this systematic review will reveal a comprehensive description of the benefits and risks of CINV antiemetic agents used in hematologic patients receiving HEC or MEC within conditioning protocols for HSCT, as well as the most appropriate combination of these drugs for different conditioning regimens.
As a result, this systematic review could be of great importance for patients dealing with the consequences of CINV in order to improve their quality of life, as well as for healthcare professionals responsible for providing care to hematological patients undergoing HSCT.
Authorship statementNBG and PSC wrote the manuscript. MAPM, CBG and LAM contributed to the conceptualization and provided fundamental knowledges. All authors reviewed and approved the final version of the manuscript for publication.
Funding sourcesThe authors received no specific funding for this work.
Ethical considerationsThe authors declare no ethical considerations.

