

Multidrug-resistant pulmonary tuberculosis (MDR-TB) is a disease affecting pulmonary parenchyma and tracheobronchial tree due to organisms which shows high-level resistance to both isoniazid and rifampicin, with or without resistance to other anti-TB drugs. Extensively drug-resistant tuberculosis (XDR-TB) is characterized for in vitro resistance to isoniazid and rifampicin plus any fluoroquinolone and at least one injectable drug (capreomycin, amikacin or kanamycin).
In 2013, among the world reported cases of pulmonary tuberculosis, 450,000 were MDR-TB or XDR-TB. Almost 60% of them were located at India, China and Russian Federation. In Spain, in 2012, 6,046 cases of tuberculosis were reported, with a 3.9-4.3% proportion of MDR-TB; and approximately 6% of them could be XDR-TB, a higher ratio than other occidental countries. MDR-TB poses special challenges on his treatment. Curation rate is around 62% and mortality reaches 11%. Male gender, alcoholism, quinolone resistance and positive smear at diagnosis are poor prognostic factors. In XDR-TB, curation rates falls to 43.7% and mortality reaches 20.8%.
Current treatment of MDR-TB needs to be individualized, being guided by antibiogram and including in the first 6 months an injectable drug (amikacin, kanamycin, capreomycin, streptomycin) and a fluoroquinolone (levofloxacin, moxifloxacin or ofloxacin) during the complete course of treatment. Treatment should include at least 4 effective agents and should continue 18 months after obtaining negative cultures2.
Bedaquiline (Sirturo®, Lab. Janssen), is a new diarylquinoline approbed by FDA (December 2012) according to the accelerated approval pathway, intended to facilitate and expedite development and review of new drugs to address unmet medical need in the treatment of a serious or life threatening condition, based on a surrogate endpoint or an intermediate clinical endpoint and clinical benefit that can be verified by post approval studies. Bedaquiline was approved by EMA in March 2014 after an orphan drug designation in 2005.
Bedaquiline is available in 100 mg tablets. The recommended dosage is 400 mg once daily during weeks 1 and 2, and 200 mg per day three times per week (with at least 48 hours between doses) weeks 3 to 24. Bedaquiline tablets should be taken with food, in order to increase oral bioavailability (by about 2-fold). Tablets should be swallowed whole with a glass of water.
Bedaquiline efficacy and safety in children younger than 18 years and in adults older than 65 years has not been established yet. Dosage adjustment in patients with mild or moderate renal impairment is not needed. In patients with creatinine clearance < 30 ml/min, terminal renal disease requiring hemodialysis, peritoneal dialysis or mild or moderate hepatic impairment bedaquiline should be used with caution. In patients with severe hepatic impairment, bedaquiline is not recommended.
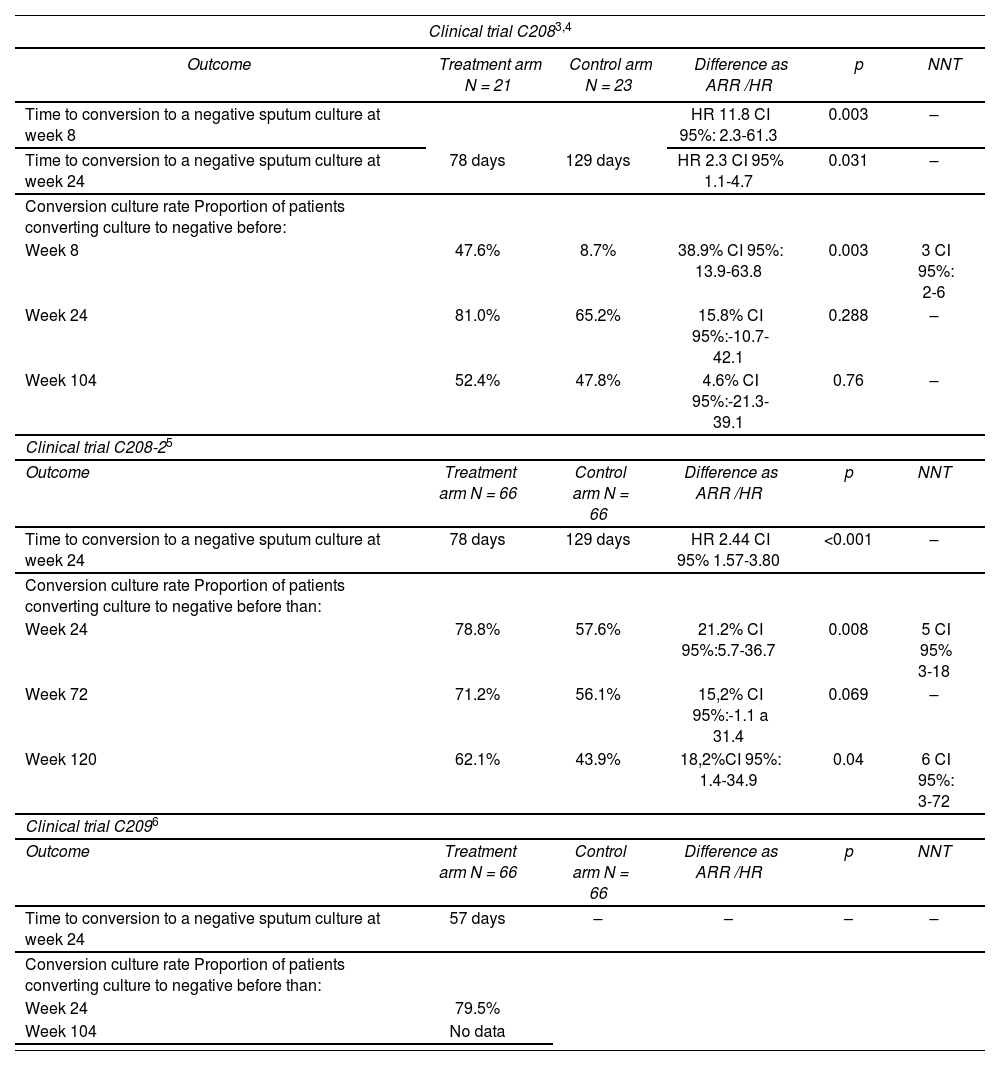
EfficacyThree clinical trials (CT) with bedaquiline in multi-drug-resistant pulmonary tuberculosis have been carried out (C208, C208-2 and C209).
Clinical trial C208 is a phase II randomized study, double blinded placebo controlled, comparing bedaquiline versus placebo when added to a standard five-drug, second-line antituberculosis regimen in MDR-TB. Trial was conducted in two consecutive stages: firstly, an exploratory stage (based on 8 weeks bedaquiline treatment followed by standard treatment for MDR-TB)3 and afterwards a stage of efficacy assessment (based on 24 weeks bedaquiline treatment followed by standard treatment for MDR-TB until 104 weeks) 4. Both stages were analyzed separately. After the double-blinded phase was finished, participants continued to receive their treatment for MDR-TB. Safety, tolerability, pharmacokinetics and microbiological efficacy were determined 96 weeks after receiving last dose of bedaquiline or placebo.
This trial was replicated with a greater sample of 161 patients and including new countries and assessing clinical response at 24, 72 and 120 weeks. Time to conversion to a negative sputum and conversion culture rate were studied. Data from this trial (C208-2) have been published recently5.
In trial C2096, open-label single arm study, 205 patients with MDR-TB or XDR-TB diagnosed ex novo or previously treated, were included. Unlike previous trials, C209 excluded VIH+ patients with CD4 < 250 cells/μL. Bedaquiline dosage was the same than in previous trials. Standard treatment was individualized according to national guidelines, with a length of 72-96 weeks and a minimum of 12 months after culture conversion.
A phase III trial with 600 patients with MDR-TB or pre-XDR-TB (resistance to fluoroquinolones or to injectable agents, but no to both agents), smear sputum-confirmed, has been recently cancelled.
Table 1 shows the main results of these trials.
Results of pivotal clinical trials with bedaquiline3-6
| Clinical trial C2083,4 | |||||
|---|---|---|---|---|---|
| Outcome | Treatment arm N = 21 | Control arm N = 23 | Difference as ARR /HR | p | NNT |
| Time to conversion to a negative sputum culture at week 8 | HR 11.8 CI 95%: 2.3-61.3 | 0.003 | – | ||
| Time to conversion to a negative sputum culture at week 24 | 78 days | 129 days | HR 2.3 CI 95% 1.1-4.7 | 0.031 | – |
| Conversion culture rate Proportion of patients converting culture to negative before: | |||||
| Week 8 | 47.6% | 8.7% | 38.9% CI 95%: 13.9-63.8 | 0.003 | 3 CI 95%: 2-6 |
| Week 24 | 81.0% | 65.2% | 15.8% CI 95%:-10.7-42.1 | 0.288 | – |
| Week 104 | 52.4% | 47.8% | 4.6% CI 95%:-21.3-39.1 | 0.76 | – |
| Clinical trial C208-25 | |||||
| Outcome | Treatment arm N = 66 | Control arm N = 66 | Difference as ARR /HR | p | NNT |
| Time to conversion to a negative sputum culture at week 24 | 78 days | 129 days | HR 2.44 CI 95% 1.57-3.80 | <0.001 | – |
| Conversion culture rate Proportion of patients converting culture to negative before than: | |||||
| Week 24 | 78.8% | 57.6% | 21.2% CI 95%:5.7-36.7 | 0.008 | 5 CI 95% 3-18 |
| Week 72 | 71.2% | 56.1% | 15,2% CI 95%:-1.1 a 31.4 | 0.069 | – |
| Week 120 | 62.1% | 43.9% | 18,2%CI 95%: 1.4-34.9 | 0.04 | 6 CI 95%: 3-72 |
| Clinical trial C2096 | |||||
| Outcome | Treatment arm N = 66 | Control arm N = 66 | Difference as ARR /HR | p | NNT |
| Time to conversion to a negative sputum culture at week 24 | 57 days | – | – | – | – |
| Conversion culture rate Proportion of patients converting culture to negative before than: | |||||
| Week 24 | 79.5% | ||||
| Week 104 | No data | ||||
ARR= Absolute Risk reduction, HR = hazard ratio, CI = Confidence Interval, p= probability, NNT= Number needed to treat.
According to the scarce trials available at this moment, bedaquiline role should be considered with caution. The subrogate endpoint used as the main outcome could limit the methodological validity. Time to culture conversion at 8 or 24 weeks is a good predictor of cure without relapse in trials of drug-sensitive tuberculosis, but this outcome has poor prognostic value for individual patients and has been not validated for MDR-TB. In addition, clinical relevance of the reduction of conversion time is not clear and may not be correlated with definitive cure6, although this concept should be reviewed8. That recommendation was based in a literature review and in two cohort studies, one of them prospective and another one retrospective3,7.
Another relevant point of interest refers to the high rate of dropouts in all the trials, reaching 42.8%3,4.
Finally, there were lack of data about cure rates as a final outcome. Post hoc assessment of trial C208-2 data based on WHO cure definition, gave a proportion of patients cured at week 120 of 57.6% in bedaquiline arm and 31.8% in placebo arm (Absolute risk reduction-ARR 25.8%; CI 95% 9.4-42.1; Number needed to treat-NNT 4; CI 95% 3-11)5,8.
SafetyThe more frequent adverse events with bedaquiline were nauseas, arthralgia, headache and vomiting. With lower frequency, dizziness, transaminases elevation, myalgia, diarrhea and QT-interval prolongation were also reported. Overall, 96.1% out of 102 patients receiving bedaquiline and 95.2% out of 105 patients in control group reported at least one adverse event6. The more severe adverse events were cardiac toxicity, hepatotoxi-city and mortality9.
Mortality pooled analysis of C208 and C208-2 trials revealed a mortality of 12 out of 102 patients (11.8%) in bedaquiline arm versus 4 out of 105 (3.8%) in placebo arm (NNH 14; CI 95% 7-334). In trial C209 16 deaths have been reported (16/233, 6.9%), four in patients dropped from trial6,10. This imbalance between deaths in both arms of trials has no explanation. Most of the deaths in bedaquiline group could be attributed to a tuberculosis progression, and did not happen during the treatment phase. In addition, this rate is near the 11% mortality rate of MDR-TB. However, this mortality increase compared to placebo is relevant enough to be considered with caution, and FDA has added a black box to the label.
Bedaquiline is biotransformed by CYP3A4. Because this, administration of bedaquiline with moderate or strong inductors (efavirenz, etravirine, rifampicin, rifapentin, rifabutin, carbamazepine, phenytoin, St John’s worth) could decrease exposition to the drug. On the contrary, bedaquiline exposition could be increased when is administered with CYP3A4 inhibitors (ketoconazole, lopinavir/ritonavir). There is no bedaquiline interactions described with nevirapin, isoniazide, pirazinamide, ethambutol, kanamycin, ofloxacin or cycloserine.
Economic areaThe average wholesale price of bedaquiline in the US market is $ 36,000 per package of 188 tablets (Red Book Online), equivalent to € 26,538 (change to June 2014). Since bedaquiline is added to standard treatment of MDR-TB, the incremental cost of the drug will be € 26,538 per treatment. The incremental cost effectiveness can be seen in Table 2.
Incremental cost-effectiveness ratio of bedaquiline
| Reference | Outcome variable | Bedaquiline | Placebo | Effectiveness difference (95% CI) | Incremental cost | ICER (95%CI) per additional cured patient |
|---|---|---|---|---|---|---|
| Clinical trial C208-24,5,9 | % cured | 57.6% | 31.8% | 25.8% (CI 95% 9.4-42.1) NNT 4 (CI 95% 3-11) | 26,538 € | 106,152 € (95% CI 79,614-291,918) |
NNT = Number needed to treat, ICER = Incremental Cost-effectiveness ratio
Assuming cure rates in Table 2, and accepting 11% of mortality in cured patients11, the difference in mortality for bedaquiline would be 2.85 deaths (6.34 minus 3.49). Therefore, with bedaquiline 2.85 deaths were avoided for every 100 patients during the treatment of MDR-TB. However, it is necessary to consider that the trial found 9.1% mortality with bedaquiline and 1.5% mortality with placebo. Considering these data, the beneficial effect of reducing mortality due to bedaquiline therapeutic effect can be offset, so that, paradoxically, get fewer years of life gained, or QALYs with bedaquiline. Therefore, before calculating the ICER in € / QALY is necessary to clarify the increased mortality observed in the clinical trial for bedaquiline arm.
According to incidence data cited above, bedaquiline potential budgetary impact in Spain would occur on a range from newly diagnosed cases (4.25% of 5,367 patients = 228), population studied in trials to the global population with TB-MDR (4.25% of 6,046 = 257), assuming that all patients were treated. Assuming the above costs and adherence of 100%, the treatment of MDR-TB would increase statewide between € 5,577,792 and € 6,287,248. From a pragmatic point of view, and considering that dropouts in the clinical trial at 24 weeks were 10% (reaching 50% at 104 weeks), these figures may be somewhat reduced.
Additional considerationsCurrently available evidence about the role of beda-quiline in MDR-TB has low quality, but the available results of phase II clinical trials suggest that this drug might contribute to achieving the objectives of the WHO about TB treatment. Although WHO, FDA and certain civil organizations have urged Janssen Laboratories to conduct phase III clinical trials in order to define more clearly and with more quality bedaquiline positioning in the treatment of tuberculosis, this is still a desideratum and there is no clinical trial registered to be conducted of these outstanding features in the meta-CT records.
Bedaquiline, added to its limited efficacy, provides more than uncertain safety data. The drug has some serious but uncommon side effects such as QT prolongation and a possible impairment of liver function. The limited size of populations treated in trials makes it difficult to objectively estimate the risk to develop these adverse effects. We may remind that to detect a 90% chance an adverse reaction with an incidence of 1/100 a drug must be given to at least 300 patients. The cardiovascular safety of bedaquiline has been studied only in 394 patients.
More worrying is the subject of increased mortality with bedaquiline. As seen before, the difference in mortality between the active and control groups (11.8% vs. 3.8%, Number needed to harm-NNH 14, 95% CI 7-334) is relevant enough to consider it significant. If we consider cure rates according to WHO criteria (57.6% vs. 31.8%, NNT 4 CI 95% 3-11) criteria, we can calculate the LHH (likelihood of Being Helped versus harmed, possibility of being helped against being harmed) defined as (1 / NNT) / (1 / NNH). In our case, this value would be given by (1/4) / (1/14) = 3.5, that is, for every 3.5 cured patients with bedaquiline one death occurs. With all the caveats of prematurity of data, these outcomes are really disturbing.
Conclusion - Therapeutic Positioning and conditions of useIn view of the results of efficacy and safety, the proposed positioning is considered Category A-1 (category explanation is included in MADRE program1): NOT INCLUDED IN THE FORMULARY because it is not possible to evaluate the drug appropriately due to insufficient information in the application. Therefore, it is suggested not to fund bedaquiline widely awaiting the results of the phase III CT requested and further safety analysis. However, the drug should be available in a very controlled manner in the context of special access programs for the treatment of MDR tuberculosis, linking funding to the generation of evidence or the achievement of clinical results previously agreed.
This paper is an abstract of bedaquiline drug evaluation report by GENESIS-SEFH (Group for Innovation, Assessment, Standardisation and Research in the Selection of Drugs of the Spanish Society of Hospital Pharmacy) that can be retrieved in his entire form from GENESIS web (http://gruposdetrabajo.sefh.es/genesis/). This evaluation has been made with the aid of MADRE 4.0 application1.

