



Pediatric palliative care aims to provide a professional, scientific, and compassionate response to the needs of terminally ill pediatric patients, with pain management being one of its fundamental pillars. This systematic review analyzes the ethical aspects involved in the management of pain in pediatric patients at the end of life, using the core principles of clinical bioethics: autonomy, beneficence, non-maleficence, and justice as a framework.
Materials and methodsA systematic review was conducted following the guidelines of the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement. Original qualitative or quantitative studies published between 2010 and 2024 in English or Spanish were included, provided they addressed pain management in pediatric palliative care from an ethical perspective. The databases consulted were PubMed, Scopus, and Web of Science. Methodological quality was assessed using the Mixed Methods Appraisal Tool (MMAT).
ResultsA total of 18 studies met the inclusion criteria. Autonomy was addressed in a limited manner, often through indirect participation of the child via their caregivers. The principles of beneficence and non-maleficence were compromised by the underuse of analgesics due to fear of adverse effects, delays in referral to palliative care, and the continuation of futile treatments. The principle of justice was reflected in structural barriers, unequal access to opioids, and limited availability of specialized care, particularly in resource-limited settings.
ConclusionsBioethical principles are present in the management of terminal pediatric pain, but their application remains inconsistent. There is a clear need to enhance professional training, implement standardized clinical protocols, and promote effective communication with families.
los cuidados paliativos pediátricos intentan dar una respuesta profesional, científica y humana a las necesidades del paciente pediátrico en fase terminal, siendo el control del dolor uno de sus pilares fundamentales. Esta revisión sistemática analiza los aspectos éticos implicados en el manejo del dolor en pacientes pediátricos en situación terminal, tomando como referencia los principios fundamentales de la bioética clínica: autonomía, beneficencia, no maleficencia y justicia.
Material y métodosse realizó una revisión sistemática siguiendo las directrices de las guías PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses). Se incluyeron estudios originales, cualitativos o cuantitativos, publicados entre 2010 y 2024 en inglés o en español, que abordaran el manejo del dolor en cuidados paliativos pediátricos desde una perspectiva ética. Las bases de datos consultadas fueron PubMed, Scopus y Web of Science. La calidad metodológica se evaluó mediante la herramienta MMAT (Mixed Methods Appraisal Tool).
Resultadosse seleccionaron 18 estudios que cumplían los criterios de inclusión. La autonomía se abordó de forma limitada, con una participación indirecta del menor a través de sus cuidadores. La beneficencia y la no maleficencia se vieron comprometidas por el uso limitado de analgésicos por temor a efectos adversos, el retraso en la derivación a cuidados paliativos y la persistencia de tratamientos fútiles. El principio de justicia se reflejó en barreras estructurales, en el desigual acceso a opioides y a cuidados especializados, especialmente en contextos con recursos limitados.
Conclusioneslos principios bioéticos están presentes en el abordaje del dolor pediátrico en situación terminal, pero su aplicación es heterogénea. Se destaca la necesidad de mejorar la formación profesional, establecer protocolos clínicos claros y fomentar una comunicación efectiva con las familias.
Each year, between 900 and 1500 children and adolescents die in Spain. Although infant mortality has decreased, the prevalence of incurable diseases and disabilities has increased. In the first year of life, congenital malformations, deformities, and chromosomal abnormalities are the most common causes of death. Patients with these conditions are the most likely to receive paediatric palliative care (PPC). After the first year, cancer and neurodegenerative diseases are the most common causes of death.1
In 2002, the World Health Organisation defined PPC as “active total care of children's body, mind and spirit, including support for the family. It begins when a life-threatening illness is diagnosed and continues regardless of whether or not children receive treatment for the illness itself, without being exclusive”.2 The aim of PPC is to improve the quality of life of children, adolescents, and their families when no treatment can substantially alter the course of the illness.2 The aim of PPC is not to cure, but rather to provide care that maximises the patient's well-being.3
The symptoms experienced by PPC patients are wide-ranging and varied. Pain is the most common symptom, causing the greatest levels of anxiety in children, their families, and those around them. It has been estimated that more than 70% of PPC patients experience some degree of moderate to severe discomfort, which reduces their quality of life.4 When addressing physical suffering in children and adolescents, the goal should always be to improve their quality of life by taking into account their emotional, family, and spiritual needs. In many cases, achieving complete pain relief is effectively impossible. Thus, the goal is to maximise well-being, while balancing symptomatic pain control with the adverse effects of the drugs used.5,6
The most common ethical problems in PPC are related to the process of making end-of-life decisions. This is a complex issue because, in most cases, children cannot act independently, so their parents or guardians act as their representatives.7 In this context, children are at the centre of all decisions, with the goal of choosing the option that will be the most beneficial.8 Both families and healthcare professionals play a key role in empowering children and encouraging their participation in matters related to their health. Another relevant ethical dilemma in the field of PPC concerns the communication of bad news.9 These ethical issues can be addressed by applying the 4 principles of clinical bioethics: autonomy, beneficence, nonmaleficence, and justice. These principles provide both a structured approach and a solid basis for analysing the moral aspects of clinical decisions relating to pain management in children.10
In recent years, the paradigm of paediatric healthcare has shifted from a model focussing solely on protecting minors to one that progressively recognises their rights according to their level of maturity and understanding.7 This change directly affects how sensitive clinical decisions are approached, such as those related to pain management in the terminal stage, where numerous ethical dilemmas arise. Given this background, this study aimed to analyse the ethical aspects of pain management for paediatric patients in terminal situations, drawing on the fundamental principles of clinical bioethics.
Material and methodsReview designWe conducted a systematic review and followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)11 guidelines to describe the literature search and the inclusion or exclusion of studies. The information obtained from the various databases was analysed in order to address the stated objective.
The Population, Exposure, Outcome (PEO) model was used to structure the research question.12 In this study, the population comprised terminally ill paediatric patients, their families, and healthcare professionals; exposure refers to pain management in the context of PPC; the outcome of interest focused on ethical aspects, which were analysed according to the fundamental principles of bioethics.
Although the authors checked the PROSPERO registry for similar reviews, the protocol for this review was not registered.
Eligibility criteriaInclusion criteria: original qualitative and quantitative studies that explicitly addressed ethical aspects related to pain management in terminally ill paediatric patients. Studies focusing on the perceptions of families and healthcare professionals were eligible, as well as those analysing clinical practices related to the treatment of physical suffering. Articles published in English or Spanish that were available via open access or accessible through institutional libraries were accepted. Only studies of good methodological quality—as assessed using the Mixed Methods Appraisal Tool (MMAT) version 2018,13—were included, with the appropriate criteria applied according to the study design.
Exclusion criteria: Studies that required a financial outlay for access were excluded, as were all articles that did not focus on the study objective.
Search strategyThe search included publications from January 2010 to December 2024. Information needed to meet the objectives was obtained from the Scopus, PubMed, and Web of Science databases.
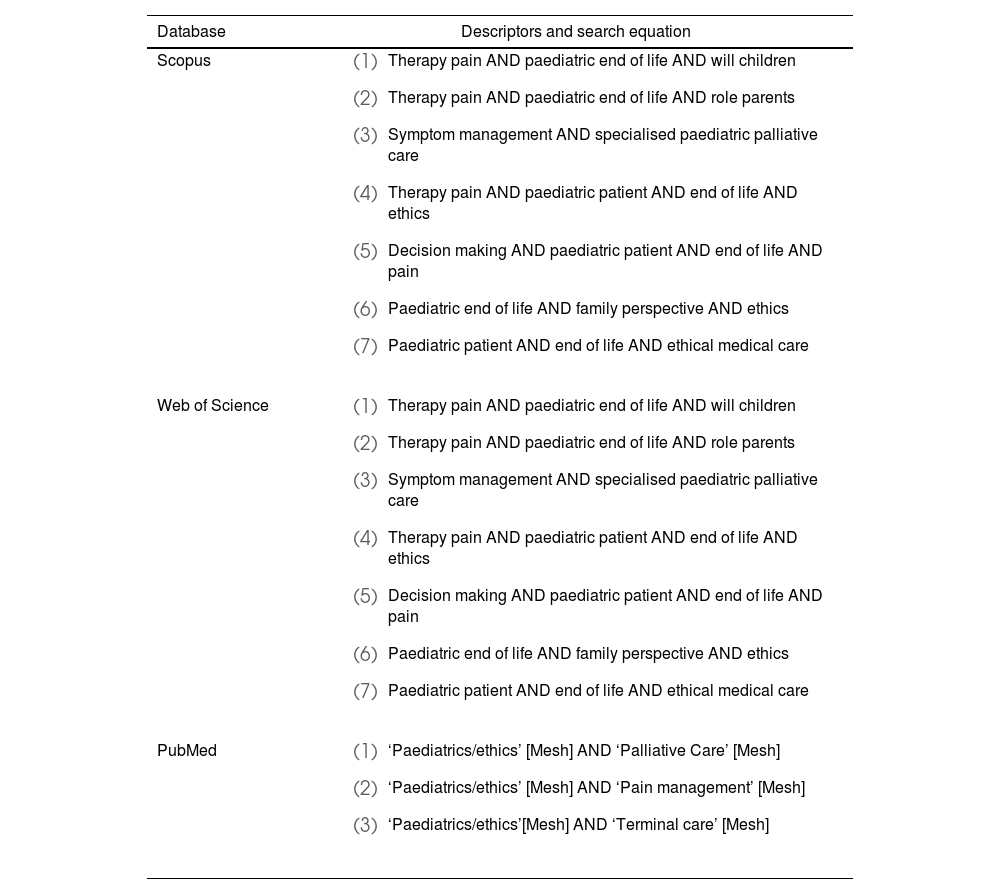
For the search strategy, MeSH terms were used in PubMed, while free-text keywords were employed in Scopus and Web of Science, with terminology adapted to the specific characteristics of each database. The terms were combined using Boolean operators to optimise the retrieval of relevant studies. The following terms were used: ‘pain,’ ‘palliative care,’ ‘terminal care,’ and ‘ethics,’ as well as complementary expressions, including ‘paediatric end of life,’ ‘will children,’ ‘role parents,’ and ‘decision making.’ Two researchers independently conducted the search and selection procedure. Table 1 shows the literature search strategy.
Databases and search equations used.
| Database | Descriptors and search equation |
|---|---|
| Scopus |
|
| Web of Science |
|
| PubMed |
|
The methodological quality of the included studies was assessed using the MMAT13 tool, with the relevant criteria applied based on the study design. Studies that met at least 3 of the 5 methodological criteria and did not have any serious deficiencies that compromised the validity of the results were considered appropriate.
ResultsThe literature search yielded 244 articles, of which 18 met the inclusion criteria, as shown in the PRISMA flow diagram (Fig. 1).

Table 2 summarises the main characteristics of the articles included in this systematic review.
Description of the included articles.
| Year | Author(s) | Objective | Methodology | Bioethical principles identified | Key findings related to pain | Methodological quality (MMAT) |
|---|---|---|---|---|---|---|
| 2010 | Delgado et al.14 | To conduct a survey of paediatric oncologists to assess the availability and quality of PPC services | Cross-sectional quantitative study.Structured questionnaire administered to 242 PPC professionals | Beneficence, nonmaleficence, justice | Only 46.2% of professionals reported the availability of specialised PPC services and 63.1% reported access to pain management. 66% reported difficulties in obtaining opioids. Only 57% of professionals in low-income countries considered pain control to be effective, compared to 87% in high-income countries (P < .001). 41.2% stated that they did not have enough time to provide quality PPC. | 3/5 (moderate) |
| 2015 | Jagt-van Kampen et al.15 | To describe the timing, duration, and management of symptoms in children with incurable brain tumours during the palliative phase | Retrospective quantitative study.Review of medical records of 34 paediatric patients diagnosed with incurable brain tumours | Beneficence, nonmaleficence | 91.2% experienced pain, with a mean duration of 43 days until death. 64.7% experienced headache; 17.6% experienced back/neck/leg pain, 2.9% experienced facial pain, and 2.9% experienced abdominal pain. 38.2% received parenteral morphine, with a median duration of use of 4 days; 23.5% were sedated with midazolam. 97.1% of parents considered the pain treatment to be appropriate. | 4/5 (high) |
| 2015 | Van der Geest et al.16 | To explore the importance of faith and hope as coping mechanisms during the paediatric palliative phase and their relationship with the long-term psychological adjustment of parents after the death of their child | Retrospective quantitative study.Structured questionnaire administered to 89 parents of children who died of cancer | Autonomy, beneficence | 65.2% of parents expressed hope that their child would die without pain. Hope for a cure (34.7%) or religious beliefs (21.3%) made it difficult to accept interventions focused exclusively on alleviating suffering. The expectation of a painless death was accompanied by doubts about palliative care, creating ethical tensions in clinical decision-making | 4/5 (high) |
| 2016 | Ullrich et al.17 | To assess whether PPC influenced the type and quality of end-of-life care in children who died after a HAT | Retrospective quantitative study.Review of medical records of 147 children who died after a HAT | Beneficence, nonmaleficence, justice | Among children who received PPC (n = 37; 25.2%), pain management was documented in 78.4% of cases, compared to 44.0% in the group without PPC (P < .001). The use of opioids was also more frequent in the PPC group (97.3% vs 66.7%; P < .001). Despite the benefits, the initiation of PPC was delayed by a median of 0.7 months prior to death | 4/5 (high) |
| 2016 | Vollenbroich et al.18 | To analyse the perceptions of parents and healthcare professionals regarding symptoms and the quality of symptomatic treatment during home PPC. | Mixed, retrospective study.Structured questionnaire administered to 38 parents of children who died after receiving home PPC. | Beneficence, nonmaleficence | 57.9% of parents reported pain as the most frequent symptom and 84.6% rated the treatment as successful. Accurate perception of pain by the medical team was significantly correlated with better treatment quality (P < .0001) and greater parental satisfaction (P = .037). Successful symptomatic treatment was reported in 71.1% of cases | 4/5 (high) |
| 2018 | Esmaili et al.19 | To describe the structural, cultural, and communication barriers to PPC in Tanzania | Prospective qualitative study.Semi-structured interviews with 14 healthcare professionals and 20 carers of terminally ill children with cancer | Beneficence, nonmaleficence, justice | 65.0% of carers reported that their children experienced pain, but only 20.0% of children themselves actively expressed this using the Wong-Baker FACES Pain Rating scale. Although 57.1% of staff stated that morphine was useful, 50.0% said that it was often out of stock or inaccessible. Cultural stigmatisation of pain and lack of effective clinical communication exacerbated suffering | 4/5 (high) |
| 2019 | Zernikow et al.20 | Retrospective evaluation of the care received by deceased children and the impact of access to specialised PPC based on 3 time cohorts (2000, 2005, and 2010) | Quantitative, retrospective study.Semi-structured interviews with 124 parents of children who died of cancer | Beneficence, nonmaleficence | Between 71% and 85% of parents reported that their child experienced pain during the final stage of the disease. This symptom was treated in 95–100% of patients, although only 53–57% of parents considered the treatment to be effective. Along with dyspnoea, pain was one of the symptoms most frequently perceived as distressing.aThe range of percentages is due to the variations observed among the 3 cohorts analysed (2000, 2005 and 2010). | 5/5 (high) |
| 2020 | Araújo Affonseca et al.21 | To describe a 5-year experience with palliative extubation in a paediatric intensive care unit, including clinical characteristics and outcomes | Quantitative, retrospective study.Review of medical records of 19 patients with severe neurological diseases undergoing palliative extubation | Beneficence, nonmaleficence | After palliative extubation, 57.9% of patients died in hospital. 73.7% received prior sedation or analgesia (42.1% received morphine, 26.3% received midazolam, with some receiving scopolamine or atropine as adjuncts). No symptoms of discomfort were observed in 8 patients after extubation. Pain control was considered effective, with no signs of acute, untreated suffering reported. | 4/5 (high) |
| 2020 | Leemann et al.22 | To analyse the differences between mothers and fathers in the care needs of children in the final stage of life. | Quantitative, retrospective study.Structured questionnaire administered to 156 parents of 78 deceased children. | Beneficence, nonmaleficence | Both parents prioritised participation in decision-making (median: 7; range: 1–7). Mothers rated needs higher than fathers on 82% of items. Two items showed statistically significant differences (P ≤ .001). Mothers placed a higher value on the use of non-pharmacological measures to relieve pain. Fathers placed greater importance on the children's interactions. The differences between mothers and fathers related to family support, reflecting gender-specific caregiving and coping roles | 4/5 (high) |
| 2021 | Mekelenkamp et al.23 | To evaluate access to, the use of, and the impact of specialised PPC in children who received HAT | Retrospective quantitative study.Review of medical records of 233 deceased children and structured survey of 41 healthcare professionals from HAT units | Beneficence, nonmaleficence, justice | Pain was one of the most frequent symptoms in the last week of life, affecting 79.0% of patients. However, only 57.1% of patients were assessed using a standardised scale. Patients who received care from a specialist PPC team were significantly more likely to undergo pain assessment using scales (P < .001) and have pain relief documented. | 5/5 (high) |
| 2022 | Greenfield et al.24 | To identify barriers and facilitators in paediatric pain management in community palliative care from the perspective of healthcare professionals | Qualitative cross-sectional study.Semi-structured interviews with 29 healthcare professionals with experience in PPC | Beneficence, nonmaleficence | All healthcare professionals identified pain as a priority symptom. Barriers included dosage errors, lack of paediatric formulations, and poor training. The use of high-dose opioids was a cause of concern due to the risk of shortening life. The use of patient-controlled analgesia and pre-filled syringes was cited as facilitators. | 5/5 (high) |
| 2022 | Andersen et al.25 | To investigate how Canadian intensive care physicians perceive the impact of the legalisation of medically-assisted dying on end-of-life care in ICUs | Prospective descriptive quantitative study.Structured questionnaire administered to 150 intensive care physicians (50% paediatric) | Nonmaleficence | All of the intensivists (including paediatricians) reported using opioids to relieve pain and dyspnoea at the end of life. 33.3% acknowledged that these drugs can hasten death, but justified their use based on the principle of double effect. 2.7% considered this use equivalent to euthanasia or murder. | 4/5 (high) |
| 2022 | Rubić et al.26 | To investigate the experiences and perspectives of medical staff regarding end-of-life decision-making in paediatric and neonatal intensive care units | Prospective qualitative study.Semi-structured interviews with 41 healthcare professionals (20 doctors and 21 nurses) | Autonomy, beneficence, nonmaleficence, justice | All of the professionals agreed that pain relief and terminal sedation are essential at the end of life. Differences were identified between doctors and nurses in the assessment of pain and the absence of clear protocols. Parental involvement is limited and tensions are evident between prolonging life and avoiding harm. | 4/5 (high) |
| 2022 | Zahedi et al.27 | To investigate ethical challenges in PPC from the perspective of Iranian paediatricians | Prospective qualitative study.Semi-structured interviews with 15 paediatric oncologists | Beneficence, nonmaleficence, justice | All participants identified pain relief as an essential ethical duty. 93.3% expressed concern about unnecessary suffering, and 80.0% mentioned cultural barriers to the use of opioids | 4/5 (high) |
| 2023 | Ridley et al.28 | To investigate continuous deep sedation practices in PPC | Retrospective quantitative study.Review of medical records of 6 adolescents/young adults diagnosed with terminal illness | Beneficence, nonmaleficence, justice | 50.0% of patients requested continuous deep sedation due to refractory pain. 66.7% of patients woke at least once during sedation, 50.0% of whom were agitated upon awakening. | 4/5 (high) |
| 2023 | Root et al.29 | To describe the reasons for patients being initially referred to the PPC team, and the issues addressed during the initial consultations | Retrospective quantitative study.Review of medical records of 56 minors diagnosed with advanced cancer | Beneficence | 55.4% of patients were referred to PPC with an indication for pain management. During the first consultation, pain was discussed in 85.6% of cases. At follow-up visits, pain was discussed again in 78.6% of cases. It was the most frequently addressed issue in all phases of follow-up | 5/5 (high) |
| 2023 | Stoesslein et al.30 | To describe the clinical and care characteristics of patients treated in a hospital PPC unit | Quantitative, retrospective study.Review of 487 admissions of 201 children with advanced disease | Beneficence, nonmaleficence | At admission, 54.0% of patients had acute pain as a clinical symptom requiring intervention. In the oncology subgroup (n = 36), 88.9% had acute pain. After dyspnoea (61.0%), pain was the second most frequent acute symptom. In addition, 58.3% of patients had more than 2 acute symptoms | 5/5 (high) |
| 2024 | Lu et al.31 | To analyse the experience of paediatric clinicians in end-of-life care and to identify the different educational needs of doctors and nurses, as well as any associated factors | Quantitative, cross-sectional, descriptive study.Structured questionnaire administered to 187 healthcare professionals (52 doctors and 135 nurses) in paediatric and neonatal ICUs | Autonomy, beneficence, nonmaleficence, justice | Pain management was reported as one of the highest priorities regarding educational needs. It was classified as a priority topic (range 1–4) by 75.0% of doctors. This priority was significantly higher among clinicians with more experience in end-of-life care (87.0% vs 72.6%; P = .018). More-experienced clinicians also placed greater importance on communicating with families regarding the ineffectiveness of treatment and ethical decision-making | 3/5 (moderate) |
PPC, paediatric palliative care; HAT, haematopoietic transplantation; ICU, intensive care unit; MMAT, mixed methods appraisal tool.
The ethical aspects of pain management for terminally ill paediatric patients were analysed according to the 4 fundamental principles of bioethics.
AutonomyThree studies explicitly investigated dilemmas related to autonomy in pain management. All of them described difficulties in shared decision-making between professionals and families, particularly when values, beliefs, or expectations regarding the clinical course differed.16,26,31
Van der Geest et al.16 found that certain family beliefs could lead parents to reject interventions specifically aimed at pain relief. Rubić et al.26 documented ethical conflicts arising from some caregivers' resistance to discontinuing treatments that prolonged children's suffering, even in clinical situations with an irreversible prognosis. Lu et al.31 suggested that limited training in clinical communication among healthcare personnel complicates shared decision-making in complex situations.
The studies did not focus primarily on the autonomy of paediatric patients. Esmaili et al.19 indirectly collected information on the children's perception of pain by conducting interviews with caregivers and professionals, without the children's direct participation in clinical decision-making. Ridley et al.28 noted that the suffering expressed by children was one of the reasons for indicating continuous deep sedation. However, the study did not focus on autonomy, as the children's participation in the decision was not investigated and their ability to understand the situation was not assessed.
Beneficence and nonmaleficenceAll of the included studies explicitly addressed ethical issues related to the principles of beneficence and nonmaleficence in managing pain in terminally ill paediatric patients.
Several studies investigated family members' perceptions of the effectiveness of pain control, yielding highly heterogeneous results. Some studies reported high levels of satisfaction, with ratings approaching 97%,15,18 whereas others reported lower levels of around 50%.14,20
Several studies highlighted the concerns of professionals regarding the use of deep sedation or high-dose analgesics in terminal phases, due to the risk of shortening life or causing adverse effects.24,25,28 These concerns created conflicts between the aim of pain relief and the fear of causing harm. Ullrich et al.17 and Mekelenkamp et al.23 suggested that the late initiation of PPC hindered appropriate pain management, particularly for patients experiencing severe suffering, thereby demonstrating a failure to act with beneficence.
Other studies14,19,31 found that regulatory, cultural, or training barriers to the correct use of analgesics compromised the team's ability to alleviate suffering, potentially resulting in the simultaneous violation of both principles. Likewise, cases were identified in which the continuation of treatments with little clinical benefit increased patients' suffering, contrary to the principle of nonmaleficence.26
Zernikow et al.20 and Stoesslein et al.30 described clinical scenarios in which palliative interventions and therapeutic measures were used together, without clearly defined objectives, thereby raising ethical questions about the proportionality and adequacy of pain management.
JusticeEight studies addressed ethical conflicts related to the principle of justice, focusing particularly on inequalities in access to analgesic treatments, specialised PPC, and equitable care conditions.14,17,19,23,26–28,31
Delgado et al.,14 Esmaili et al.,19 and Rubić et al.26 reported that structural and institutional barriers hindered access to appropriate analgesic interventions, thus compromising equity in pain management. One of these studies, which was conducted in Tanzania,19 identified limitations specific to settings with fewer resources, such as the restricted availability of opioids as well as cultural barriers.
Ullrich et al.17 and Mekelenkamp et al.23 showed that delayed referral to PPC hindered appropriate pain management, resulting in inequality in the quality of care. Lu et al.31 identified training gaps among healthcare professionals that impeded equity in pain care. Zahedi et al.27 described the tension between the need to show cultural respect and the obligation to provide effective analgesia.
Finally, Ridley et al.28 investigated how the characteristics of the care environment could influence effective access to pain treatment in the terminal stage.
DiscussionThis systematic review reveals how the fundamental principles of clinical bioethics are applied to the management of pain in terminally ill paediatric patients. In the studies analysed, these principles were reflected with varying degrees of emphasis and interpretation, depending on the clinical, cultural, and organisational context.
The principle of autonomy appeared to be mainly associated with shared decision-making between healthcare professionals and families. Although the importance of involving children in this process has been emphasised—adapting their participation to their developmental level and capacity for understanding—the32,33 studies analysed show that such involvement usually occurs indirectly, mediated by parents or carers. Some studies also found that shared decision-making was hindered by cultural and communication barriers, which have been widely documented in the scientific literature.34,35
The principles of beneficence and nonmaleficence were primarily evident in the tension between the duty to alleviate suffering and the fear of causing adverse effects or hastening the process of death. This ethical dilemma was particularly relevant in managing pain in terminally ill children, where the administration of potent analgesics, such as opioids, can raise concerns about the risk of respiratory depression or excessive sedation.36,37
Several of the included studies highlighted situations in which a lack of specific PPC training and clear protocols led to suboptimal pain treatment administration, thus compromising the principle of beneficence.14,19,31 Such shortcomings have also been noted in the wider literature, where insufficient professional training is recognised as one of the main barriers to effective pain management.38 These authors emphasised that a lack of training is often associated with a sense of insecurity when facing complex conversations, as well as difficulties in identifying refractory symptoms.
On the other hand, the principle of nonmaleficence may be compromised in situations when treatments that offer little clinical benefit are continued, thereby exacerbating the patient's suffering. Although not a central finding in all the included studies, some described the difficulty of limiting prolonged medical interventions due to caregiver refusal.26 The literature has acknowledged that this type of clinical decision can be problematic and has warned against therapeutic obstinacy in contexts of high uncertainty or emotional pressure.39,40
The principle of justice was mainly reflected in the identification of structural barriers hindering equitable access to analgesic treatments and specialised PPC. Some authors observed that shortages of opioids, coupled with certain cultural factors, can hinder access to appropriate care, particularly in settings with limited resources.19,27 Such inequalities have been widely documented in recent literature, which warns of inequity in access to PPC based on geographical location, socioeconomic status, or availability of care resources.41,42
This study has a number of limitations. Firstly, the limited availability of publications related to palliative care in the paediatric population made it difficult to find results that answered the objectives of this study. Furthermore, the sample size of the included studies was generally small, except for studies that took into account the perceptions of healthcare professionals. Finally, the broad eligibility period of the included studies may have introduced variability in the obtained results due to changes in PPC over the years.
The study's strengths include the use of the PEO12 model, which enabled the research question to be defined clearly and the review process to be structured. It addressed a clinically and ethically complex issue through a structured framework, using the 4 principles of bioethics to guide the analysis. In addition, the inclusion of both quantitative and qualitative studies enriched the interpretation of the results by integrating objective data with the experiences and perceptions of patients, families, and professionals. In this regard, the small sample sizes of some qualitative studies do not represent a significant methodological limitation, as these types of designs typically yield sufficient information from a limited number of participants.
In conclusion, the fundamental principles of bioethics are applied to pain management for terminally ill paediatric patients, albeit with varying degrees of development and application. Although shared decision-making with families is a central ethical principle, the direct participation of children was scarce or non-existent. There are frequent tensions between the obligation to alleviate suffering and the fear of causing adverse effects through the use of opioids or deep sedation. In addition, structural, training, and organisational barriers that hinder equitable access to PPC persist. These results highlight the need to improve specific PPC training, establish clear action protocols, and foster clinical environments that facilitate communication with families and, where possible, the patients. A structured ethical approach is essential for guiding complex clinical decisions and ensuring that care focuses on the best interests of the children.
Contribution to the literatureThis systematic review applies the fundamental principles of clinical bioethics to provide an update on the ethical dilemmas in pain treatment for children receiving paediatric palliative care. The study identifies the key barriers to providing ethical and appropriate care by integrating the available evidence and considering the perceptions of both professionals and families.
AuthorshipBoth authors contributed substantially to the study conception and design, data analysis and interpretation, and writing the article. Both read and approved this version of the manuscript. Specifically, Cristina Casanova Martínez: study design, data collection, interpretation of results, and writing the article. Mónica Gayoso Rey: interpretation of results, and writing and revision of the article.
FundingNone declared.
CRediT authorship contribution statementCristina Casanova-Martínez: Writing – original draft, Validation, Methodology, Investigation, Data curation, Conceptualization. Mónica Gayoso-Rey: Writing – original draft, Validation, Methodology, Formal analysis.
None declared.

