
To evaluate the experience of HIV+ patients with pharmaceutical care based on the ability-motivation-opportunity methodology.
MethodCross-sectional, unicentric study. The participants included were HIV+ patients attended during November-2016 and to whom the IEXPAC questionnaire was conducted. This validated questionnaire allows to know the experience of chronic patients about the health care they receive.
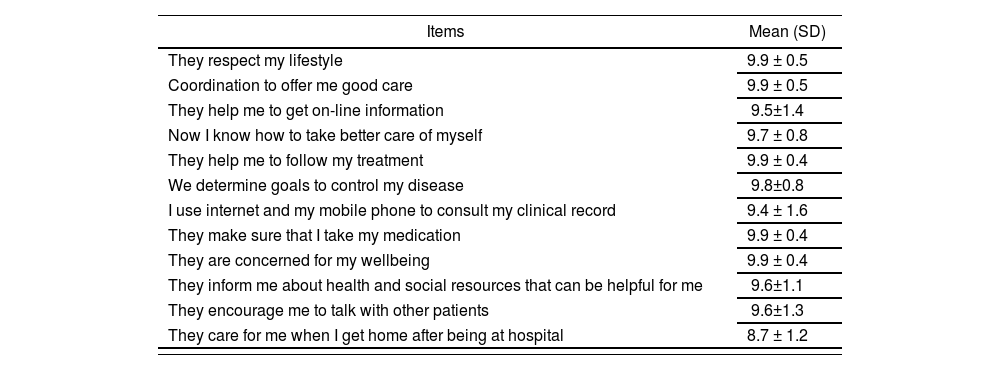
Results91 patients were included. The overall mean score of the IEXPAC questionnaire was: 9.7 ± 0,3. The items that obtained higher scores were: respect lifestyle (9.9 ± 0.5); coordination to offer good care (9.9 ± 0.5); helping to continue treatment (9.9 ± 0.4); making sure that I take medication (9.9 ± 0.4); worried about well-being (9.9 ± 0.4). The points with the possibility of improvements included: worried about me when I get home after being in hospital (8.7 ± 1.2).
ConclusionsThe evaluation of the pharmaceutical care process based on the ability-motivation-opportunity model achieve a high level in each of the identified points of interaction.
Evaluar la experiencia de pacientes VIH+ con la atención farmacéutica basada en la metodología capacidad-motivación-oportunidad.
MétodoEstudio transversal, unicéntrico, que incluyó pacientes VIH+ que fueron atendidos en noviembre de 2016 y a los cuales se aplicó el cuestionario validado IEXPAC. Este permite conocer la experiencia de pacientes crónicos sobre la atención sanitaria que reciben.
ResultadosSe incluyeron 91 pacientes. La puntuación media global obtenida fue: 9,7 ± 0,3. Los ítems que obtuvieron puntuaciones más elevadas fueron: respetan mi estilo de vida (9,9 ± 0,5); se coordinan para ofrecerme una buena atención (9,9 ± 0,5); me ayudan a seguir el tratamiento (9,9 ± 0,4); se aseguran de que tomo la medicación (9,9 ± 0,4); se preocupan por mi bienestar (9,9 ± 0,4).
Los puntos con posibilidades de mejora incluyeron: se preocupan por mí al llegar a casa tras el ingreso hospitalario (8,7 ± 1,2).
ConclusionesLa evaluación de la atención farmacéutica basada en el modelo capacidad-motivación-oportunidad cumple un alto nivel en cada punto de interacción identificado.
Hospital Pharmacy has experienced a major transformation in recent years. The emergence of the Pharmaceutical Care (PhC) concept, and the healthcare reorientation towards an improvement in health outcomes, have contributed to said change1,2.
The need to improve the quality of healthcare offered has led to developing the strategical map for outpatient care by the Sociedad Española de Farmacia Hospitalaria (MAPEX), which has generated a different view of Pharmacist activities in outpatient units3.
All this has resulted in the development of a new PhC model, known as AMO (Ability-Motivation-Opportunity). The cornerstones of this model are: Ability, understood as providing individualized PhC adapted to each patient, through stratification; Motivation, in order to reach goals with drug therapy, replacing the clinical interview with a motivational interview; and finally, Opportunity, providing PhC beyond the personal consultation, through information, communication and learning technologies4.
On the other hand, it has been currently considered that there is a need for reorientation in the relationship of the patient with healthcare professionals and systems5. Patient-focused care represents a challenge that requires a different approach in order to listen to patients and use what they have to say, and to learn from their experience in order to transform the healthcare they are receiving6,7.
In our setting, the intention has always been to measure patient experience, defined as the information provided by the person about what has happened to them in their ongoing interaction with professionals and social and healthcare services, and their experience of said interaction and its outcomes8. Thus, the IEXPAC scale has appeared recently (Instrument for Assessing Patient Experience of Chronic Illness Care). This scale can be applied to chronic patients who have received health and social care during the last six months8. There are many studies assessing its use, but none regarding PhC, and specifically about HIV+ patients9–11.
The objective of this study is to evaluate the experience reported by HIV+ patients under follow-up with a PhC model based on the AMO methodology.
MethodsA cross-sectional study, including HIV+ patients (≥18-year-old), managed at the outpatient Unit for Viral Conditions of a Speciality Hospital during November, 2016, according to the AMO methodology for PhC. The study excluded those patients enrolled in clinical trials and/or those who did not sign an Informed Consent.
The interventions conducted on patients were those included in the Stratification Model for HIV Patients, and recorded in the electronic clinical record according to the AMO taxonomy 4,12.
The primary variable of the study was the mean score for the questionnaire, used to measure the experience by HIV+ patients8.
This questionnaire has been validated in Spanish for chronic patients, and it contains 11 questions plus one, for patients who have been hospitalized in the past three years. The overall score of the 11 items in the IEXPAC scale was a 0-10 value. In order to calculate this, the scores for the 11 questions were added up, and the total number was obtained by implementing the following formula: 10 x (sum of the scores for the 11 items-11)/44. The score for item 12, about hospital discharge, was reported separately, converted into a scale of 0-10.
The online IEXPAC platform: http://www.iemac.es/iexpacconverted the scores and offered automatically both results8.
The demographical variables included were: age and gender; way of transmission (sexual or parenteral), CD4+ lymphocyte level (cells/µl), plasma viral load (copies/mL) and level of PhC stratification (through the model validated for HIV+ patients, classified into High, Medium and Low)12; antiretroviral therapy prescribed, regimens prescribed concomitantly (single tablet regimens), comorbidities and comorbidity pattern (patients had to present two or more comorbidities framed into the same pattern; comorbidities were classified into: cardiological and/or metabolic, depressive and/or geriatric, mixed, or without comorbidities), number of concomitant medications (chronic use drugs prescribed for at lest 60 days), and polypharmacy (divided into four categories: medications for cardiovascular conditions, for anxiety-depression syndromes, for chronic obstructive pulmonary disease, or other medications).
The combination of drugs dispensed was obtained through the Dispensing Program for Outpatients (Dominion®). The concomitant treatment was collected through “Receta XXI“ of the Andalusian Health System. The remaining variables were obtained from the patients’ electronic clinical record.
Sample size was determined based on the mean attendance of patients to the Viral Conditions Unit during the past year. A sample of 89 patients was obtained, with a 95% level of confidence and safety, 8% accuracy, and selected 50% rate (p=0.5); the expected loss rate was 15%.
Regarding statistical analysis, the quantitative variables were expressed with mean and standard deviations or median and P25 and P75 percentiles in case of asymmetrical distributions; qualitative variables were stated with frequencies and percentages. Data normality distribution was determined based on the Kolgorov-Smirnov test. The SPSS 22.0 statistical package for Windows (IBM Corp., Armonk, NY, U.S.A.) was used for data analysis.
The study was conducted following the ethical principles for medical research in human beings by the Declaration of Helsinki (2013).
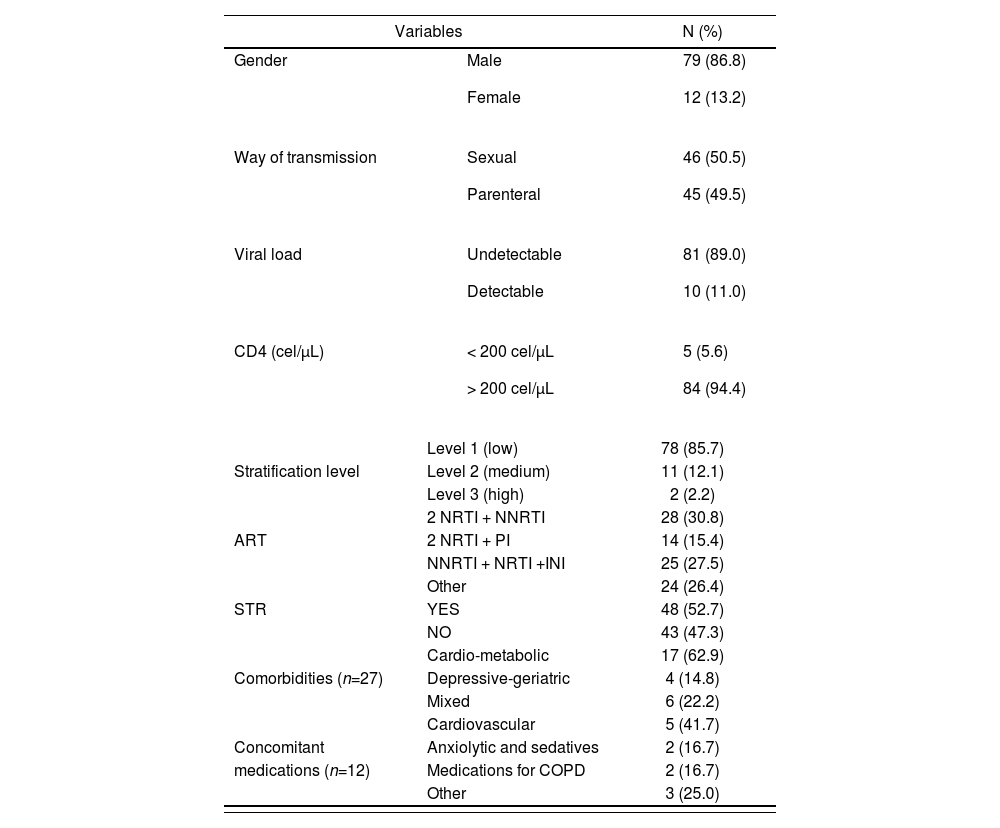
ResultsThe study included 91 patients, with 46.8±9.9 as mean age (86.8% were male). Their demographical, clinical and pharmacological characteristics are collected in Table 1.
Basal and clinical characteristics
| Variables | N (%) | |
|---|---|---|
| Gender |
|
|
| Way of transmission |
|
|
| Viral load |
|
|
| CD4 (cel/μL) |
|
|
| Level 1 (low) | 78 (85.7) | |
| Stratification level | Level 2 (medium) | 11 (12.1) |
| Level 3 (high) | 2 (2.2) | |
| 2 NRTI + NNRTI | 28 (30.8) | |
| ART | 2 NRTI + PI | 14 (15.4) |
| NNRTI + NRTI +INI | 25 (27.5) | |
| Other | 24 (26.4) | |
| STR | YES | 48 (52.7) |
| NO | 43 (47.3) | |
| Cardio-metabolic | 17 (62.9) | |
| Comorbidities (n=27) | Depressive-geriatric | 4 (14.8) |
| Mixed | 6 (22.2) | |
| Cardiovascular | 5 (41.7) | |
| Concomitant | Anxiolytic and sedatives | 2 (16.7) |
| medications (n=12) | Medications for COPD | 2 (16.7) |
| Other | 3 (25.0) | |
ART: antiretroviral therapy; INI: integrase inhibitor; NNRTI: non-nucleoside reverse transcriptase inhibitor; NRTI: nucleoside reverse transcriptase inhibitor; PI: protease inhibitor; STR: single tablet regimens.
Patients presented a mean number of 1.7±1.3 comorbidities, and the most frequent pattern was cardio-metabolic (18.7%).
The mean number of concomitant medications was 2.3±2.6; it stands out that 27.5% of patients had no medication associated. Polypharmacy pattern (five or more prescriptions) could only be calculated for 13.2% of all patients; the most frequent was cardiovascular (41.7%).
The overall mean scores of the IEXPAC questionnaires conducted was 9.7±0.3. Table 2 shows the scores for the different items.
Scores for the IEXPAC survey items
| Items | Mean (SD) |
|---|---|
| They respect my lifestyle | 9.9 ± 0.5 |
| Coordination to offer me good care | 9.9 ± 0.5 |
| They help me to get on-line information | 9.5±1.4 |
| Now I know how to take better care of myself | 9.7 ± 0.8 |
| They help me to follow my treatment | 9.9 ± 0.4 |
| We determine goals to control my disease | 9.8±0.8 |
| I use internet and my mobile phone to consult my clinical record | 9.4 ± 1.6 |
| They make sure that I take my medication | 9.9 ± 0.4 |
| They are concerned for my wellbeing | 9.9 ± 0.4 |
| They inform me about health and social resources that can be helpful for me | 9.6±1.1 |
| They encourage me to talk with other patients | 9.6±1.3 |
| They care for me when I get home after being at hospital | 8.7 ± 1.2 |
IEXPAC: Instrument for Assessing Patient Experience of Chronic Illness; SD: standard desviation.
The PhC process based on the AMO model achieved, overall, a high level of quality perceived by patients at each one of the interaction points identified. The strengths of the model were detected based on the experience of patients regarding the healthcare received. The best valuated aspects were those associated with lifestyle, coordination between healthcare professionals, and adequate take of medications. Likewise, it was detected that the item requiring the highest involvement and improvement was the one associated with Care for patients after hospitalization. Based on the scores obtained for this item, and delving into the Opportunity cornerstone of the model, an improvement in this setting could be represented by the design of new tools for contact with patients, beyond personal consultations, as well as by using the tool by Montes Escalante et al.13 in order to identify those patients at higher risk, and to avoid re-hospitalizations in HIV+ patients after discharge.
The importance of assessing patient experience has already been studied in a review conducted by Doyle et al.10, including 55 studies in total, on a high variety of conditions. Data show that patient experience is positively associated with clinical efficacy and patient safety, and this supports the importance to include patient experience among the basic cornerstones of patient care.
There is still no wide awareness about the concept of Patient Experience, and it has not been assessed in the PhC setting. There are recently published studies assessing quality perceived by patients, such as the one by Margusino-Framiñán et al.14, which studies the implementation of specialized PhC units. The result obtained at the satisfaction survey, which is an aspect different to experience, was 9.16±1.27. Along the same line, Cañamares I et al.15 also studied the experience self-reported by patients treated with direct antivirals against hepatitis C virus, where the most valued item was the contact with the pharmacist at consultation.
The main limitation of this study is that the IEXPAC questionnaire was not conducted to the whole cohort of patients at the hospital unit, but only to a cross section during November, 2016. However, the sample analyzed met the sample size required to answer all questions stated, due to the type of study and questionnaire characteristics.
Future lines of research will allow us to delve into the improvement of the experience with the AMO model, according to the different stratification levels and interventions conducted in each of them, through a prospective study.
In conclusion, the evaluation of the experience reported by HIV+ patients, through the IEXPAC questionnaire, with the AMO model for PhC, offered high scores.
FundingNo funding.
Conflict of interestsNo conflict of interests.

