


to determine the incidence of linezolid-induced haematological toxicity and study the influence of renal clearance on its appearance and the preventive effect of pyridoxine.
Methoda retrospective observational study was conducted. Every patient treated with linezolid in a university hospital during 6 months was included. Haematological toxicity was defined as a decrease of 25% in hemoglobin, of 25% in platelets and/or 50% in neutrophils from baseline. The incidence of haematological toxicity and the percentage decrease in analytical variables were compared in patients with and without renal failure (creatinine clearance lower than 50 mL/min), using the 30 mL/min threshold, and with or without pyridoxine; using Chi -Square and U Mann-Whitney tests, respectively.
Resultsthirty-eight patients were evaluated. Sixteen (42%) presented haematological toxicity (2 due to a decrease in haemoglobin, 9 in platelets and 8 in neutrophils). Two patients (5%) discontinued treatment due to thrombocytopenia. Toxi-city incidence was similar in patients with and without renal failure, 42% vs 42%, p = 0.970, with more or less than 30 ml/min, 67% vs 40%, p = 0.369, or with or without pyridoxine, 47.8% vs 33%, p = 0.376. Patients with renal failure had a significantly greater reduction in platelet count, p = 0.0185.
Conclusionsforty-two percent of patients had haematological toxicity, being more frequent platelets and neutrophils reduction. This was not significantly higher in patients with renal failure or in those without pyridoxine. Greater reduction in platelet count was observed in patients with renal failure.
determinar la incidencia de toxicidad hematológica por linezolid. Estudiar la influencia del aclaramiento renal en su aparición y la efectividad de la piridoxina en su prevención.
Métodoestudio observacional retrospectivo de todos los pa-cientes tratados con linezolid en un hospital universitario en seis meses. Se consideró toxicidad hematológica a la disminu-ción del 25% de la hemoglobina, del 25% de las plaquetas y/o del 50% de neutrófilos al final respecto al inicio del tratamien-to. Se comparó en los pacientes con y sin fallo renal (aclara-miento de creatinina inferior a 50 mL/min), con mas o menos de 30 mL/min, y con o sin piridoxina, la incidencia de toxicidad hematológica mediante Chi-Cuadrado y la disminución en el porcentaje de variables analîticas hematológicas mediante U Mann-Whitney.
Resultadosse evaluaron 38 pacientes. Dieciséis (42%) presen-taron toxicidad hematológica (2 por disminución de hemoglo-bina, 9 de plaquetas y 8 de neutrófilos). En 2 pacientes (5%) se suspendió el tratamiento por plaquetopenia. La incidencia de toxicidad fue similar en pacientes con y sin insuficiencia renal, 42% vs. 42%, p = 0,970, con mas o menos de 30 mL/min, 67% vs. 40%, p = 0,369, con piridoxina o sin ella, 47,8% vs. 33%, p = 0,376. Los pacientes con fallo renal presentaron una reducción significativamente mayor de plaquetas, p = 0,0185.
Conclusionesun 42% de los pacientes presentó toxicidad he-matológica, mas frecuentemente disminución de plaquetas y neutrófilos. Esta no fue significativamente mayor en los pa-cientes con fallo renal, ni en aquellos sin piridoxina. Se halló mayor reducción de plaquetas en los pacientes con insuficien-cia renal.
Linezolid is a synthetic antibacterial agent within the class of oxazolidinones1–6. It is a broad spectrum antibiotic, which shows activity against gram-positive aerobic bacteria and anaerobic micro-organisms1–6. It presents bacteriostatic activity against enterococcus and sta-phylococcus, and bactericide activity against the majority of streptococcus strains6.
The indications approved by the Spanish Agency of Medicines and Medical Devices are: nosocomial pneumonia, community-acquired pneumonia, and skin and soft tissue infections1–6.
Regarding its safety profile, its main adverse reaction is haematological toxicity1–6. Thrombocytopenia has been specifically described, with an incidence between 32%7 and 45.8%8, and anaemia, with a 25% inciden-ce8. In some patients, these events have led to treatment discontinuation8–9. In other cases, adverse effects have led to the need for a blood transfusion7,10.
In clinical practice, the simultaneous administration of pyridoxine is widely used for prevention of the haematological toxicity. However, there are contradictory data regarding its efficacy, and the precise mechanism which could explain this effect is still unknown8,9,11.
On the other hand, a higher likelihood of developing haematological toxicity has been observed in those patients who present renal function deterioration9,12–15.
Given this variability in the published information, the primary objective of this study is to determine the incidence of haematological toxicity in those patients treated with linezolid in a university hospital. Also, as secondary objectives, it is intended to analyze the potential protective effect of pyridoxine administration, and the potential influence of renal function on the development of haematological toxicity.
MethodsAn observational retrospective study was designed, and it was approved by the autonomous Ethics Committee, and received the authorization and classification by the Spanish Agency of Medicines and Medical Devices.
The study included all those patients admitted in a university hospital who received treatment with linezolid by intravenous or oral administration during a period of six months.
For sample size calculation, the Plachouras et al.8 study was used as reference; this showed a 45.8% incidence of thrombocytopenia. Taking an error margin of ± 17% for the Confidence Interval of 95%, 33 patients would be necessary. It was estimated that this number of patients could be recruited within 6 months.
In order to evaluate haematological toxicity, lab test results were collected for the first and last day of treatment with linezolid. For those cases where the lab test results for these dates were not available, the test results of the day before or the day after these dates was taken as reference. Those patients who had no lab test results for the start and the end of treatment with linezolid were excluded.
The following variables were collected from the patient clinical records included in the information system of the centre:
- a.
Variables collected at initiation of linezolid treatment:
- -
Demographic data: gender, age, weight, height, Body Surface Area (BSA), Body Mass Index (BMI).
- -
Clinical data: oncologic diagnosis (yes/no), administration or not of chemotherapy within the last 6 months, administration or not of immunosuppres-sant treatment, creatinine, creatinine clearance estimated through the Cockcroft-Gault Equation (CrCl), urea, C-reactive protein, procalcitonin.
- -
- b.
Variables collected regarding treatment with linezolid and pyridoxine:
- -
Indication of the use of linezolid, linezolid dosing, linezolid dosing interval, way of administration of linezolid, pyridoxine dosing, way of administration of pyridoxine.
- -
- c.
Lab test variables collected at initiation and end of treatment with linezolid in order to assess haematolo-gical toxicity: red blood cells, haemoglobin, haemato-crit, leucocytes, neutrophils, lymphocytes, monocytes, platelets.
- d.
d) Other variables: Blood transfusions.
The database used for analysis was anonymized.
The grade of anaemia, thrombocytopenia and neu-tropenia was classified according to the 4.0 version of the Common Terminology Criteria for Adverse Events (CTCAE)16 and according to the lab test results of the last day of treatment with linezolid.
In each patient, the rate of reduction between the initiation and the end of treatment with linezolid was calculated for the haemoglobin level (HR), for the platelet count (PR) and for neutrophil count (NR).
Haematological toxicity was defined as a HR superior or equal to 25% (HRT)17, PR superior or equal to 25 % (PRT)9,11,17 and/or NR superior or equal to 50% (NRT)11.
Renal failure (RF) was defined as CrCl below 50 mL/ min. The influence of a CrCl below 30 mL/min was also evaluated.
The values of HR, PR and NR were compared between patients with and without simultaneous treatment with pyridoxine, between patients with and without RF, and between patients with CrCl above or below 30 mL/min, through the U Mann-Whitney Test. The difference in incidence of haematological toxicity between these groups of patients was analyzed through Chi-Square Test. Additionally, there was a study between the CrCl, or the duration of treatment with linezolid, and HR, PR and NR through linear regression. The Spearman Corre¬lation Coefficient for the relation between CrCl and HR, PR and NR was also analyzed. The normality of variables was studied through the Shapiro-Wilk Test. Statistical analysis was conducted with the STATA 12® program.
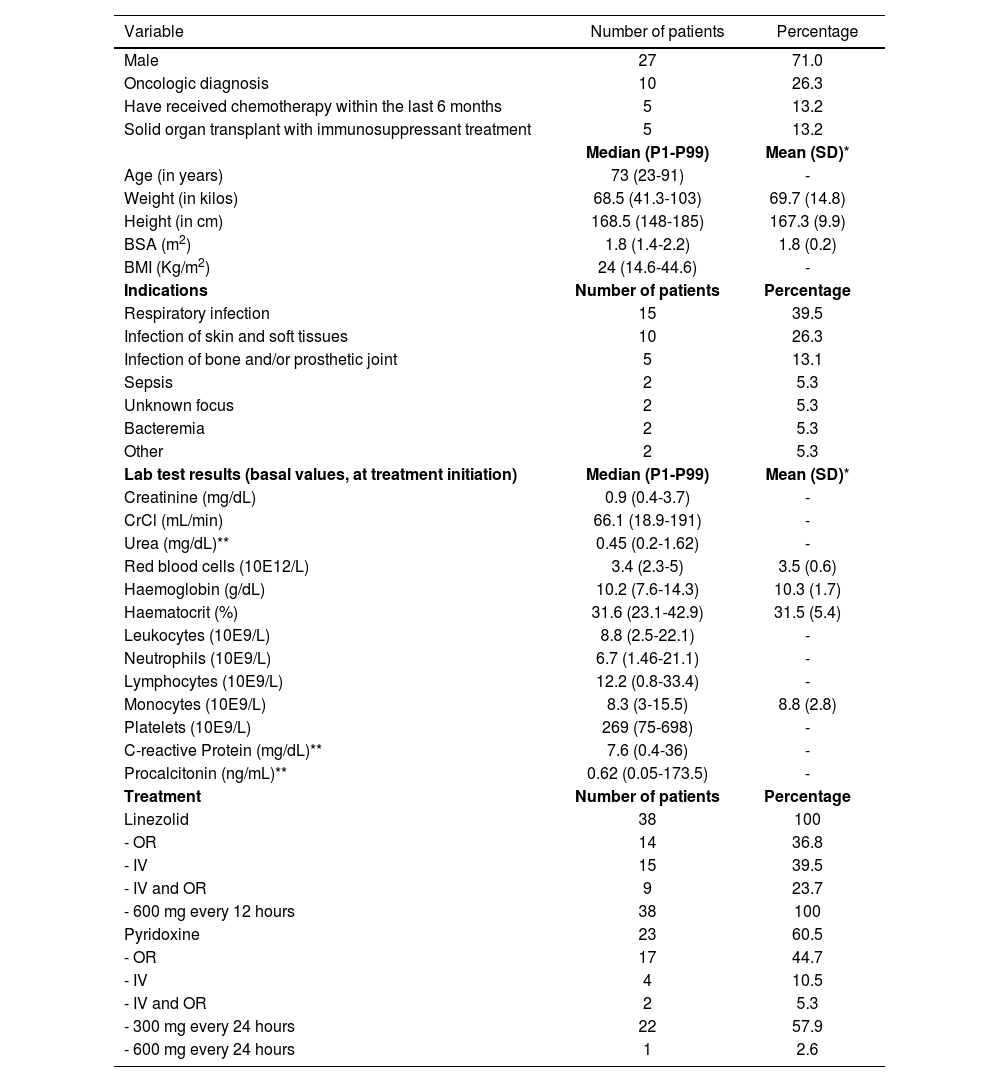
OutcomesThirty-eight (38) patients were included in the study. Table 1 shows the demographic, clinical and lab test characteristics of patients included in the study, as well as the characteristics of their treatments with linezolid and pyridoxine. Seven (7) patients were excluded, because there were no lab test results available in order to assess haematological toxicity.
Characteristics of the 38 patients included in the study
| Variable | Number of patients | Percentage |
|---|---|---|
| Male | 27 | 71.0 |
| Oncologic diagnosis | 10 | 26.3 |
| Have received chemotherapy within the last 6 months | 5 | 13.2 |
| Solid organ transplant with immunosuppressant treatment | 5 | 13.2 |
| Median (P1-P99) | Mean (SD)* | |
| Age (in years) | 73 (23-91) | - |
| Weight (in kilos) | 68.5 (41.3-103) | 69.7 (14.8) |
| Height (in cm) | 168.5 (148-185) | 167.3 (9.9) |
| BSA (m2) | 1.8 (1.4-2.2) | 1.8 (0.2) |
| BMI (Kg/m2) | 24 (14.6-44.6) | - |
| Indications | Number of patients | Percentage |
| Respiratory infection | 15 | 39.5 |
| Infection of skin and soft tissues | 10 | 26.3 |
| Infection of bone and/or prosthetic joint | 5 | 13.1 |
| Sepsis | 2 | 5.3 |
| Unknown focus | 2 | 5.3 |
| Bacteremia | 2 | 5.3 |
| Other | 2 | 5.3 |
| Lab test results (basal values, at treatment initiation) | Median (P1-P99) | Mean (SD)* |
| Creatinine (mg/dL) | 0.9 (0.4-3.7) | - |
| CrCl (mL/min) | 66.1 (18.9-191) | - |
| Urea (mg/dL)** | 0.45 (0.2-1.62) | - |
| Red blood cells (10E12/L) | 3.4 (2.3-5) | 3.5 (0.6) |
| Haemoglobin (g/dL) | 10.2 (7.6-14.3) | 10.3 (1.7) |
| Haematocrit (%) | 31.6 (23.1-42.9) | 31.5 (5.4) |
| Leukocytes (10E9/L) | 8.8 (2.5-22.1) | - |
| Neutrophils (10E9/L) | 6.7 (1.46-21.1) | - |
| Lymphocytes (10E9/L) | 12.2 (0.8-33.4) | - |
| Monocytes (10E9/L) | 8.3 (3-15.5) | 8.8 (2.8) |
| Platelets (10E9/L) | 269 (75-698) | - |
| C-reactive Protein (mg/dL)** | 7.6 (0.4-36) | - |
| Procalcitonin (ng/mL)** | 0.62 (0.05-173.5) | - |
| Treatment | Number of patients | Percentage |
| Linezolid | 38 | 100 |
| - OR | 14 | 36.8 |
| - IV | 15 | 39.5 |
| - IV and OR | 9 | 23.7 |
| - 600 mg every 12 hours | 38 | 100 |
| Pyridoxine | 23 | 60.5 |
| - OR | 17 | 44.7 |
| - IV | 4 | 10.5 |
| - IV and OR | 2 | 5.3 |
| - 300 mg every 24 hours | 22 | 57.9 |
| - 600 mg every 24 hours | 1 | 2.6 |
P1-P99: percentile 1-percentile 99; SD: standard deviation; BSA: Body Surface Area; BMI: Body Mass Index; CrCl: creatinine clearance estimated through the Cockcroft-Gault Equation; OR: oral administration; IV: intravenous administration.
All patients included in the study received a 600mg dose of linezolid every 12 hours, through oral or intravenous administration. Twenty-three patients (60.5% of all patients) also received pyridoxine for the duration of treatment with linezolid, on a 300mg daily dose through oral or intravenous administration, except for one patient who received a daily dose of 600mg. The use of pyridoxine was not included in protocols, and it increased upon publication of studies favourable to its use. The median (Percentile 1-Percentile 99) and mean (Standard Deviation (SD)) of the duration of therapy with linezolid in our population was 7.5 (1-46) and 8.4 (7.4) days, respectively.
Regarding the indications for treatment with linezolid, 15 patients (39.5%) were diagnosed with a respiratory infection, and 10 patients (26,3%) with a skin and soft tissue infection. Among the latter, the majority presented cellulitis and/or ulcer or infection of an abdominal surgical wound. The remaining 13 patients included in the study presented bone and/or prosthetic joint infection (5 patients), sepsis, bacteremia, or infection of unknown origin.
Sixteen (16 patients), 42% of those included in the study, presented haematological toxicity. A 5% of patients (2 patients) developed toxicity due to a reduction in the haemoglobin level; 24% of patients (9 patients), due to a reduction in platelets, and 21% (8 patients) due to a reduction in neutrophils. Figure 1 shows the type and frequency of toxicity observed, taking into account that some patients presented more than one type of toxicity. Out of those patients with oncological diagnosis, 4 patients (40%) presented haematological toxicity. Table 2 shows the rate of reduction in haemoglobin, platelets and neutrophils in those patients who presented haematological toxicity and those who did not present it.

Rate of reduction in cell count or haemoglobin in patients with and without haematological toxicity. Data are presented as median (percentile 1 and percentile 99) and mean (standard deviation)
| Patients with haematological toxicity N = 16 | Patients without haematological toxicity N = 22 | |||
|---|---|---|---|---|
| Median (P1-P99) | Mean (SD)* | Median (P1-P99) | Mean (SD)* | |
| HR | 30.7 (25-36.4) | - | 3.7 (-30.2-24.6) | 2.5 (13.1) |
| PR | 27.5 (25.4-62.3) | - | -3.2 (-100,4-23.1) | - |
| NR | 65 (56.8-81.4) | 66.5 (8.1) | 9.6 (-112.2-45.7) | - |
N: number; P1-P99: percentile 1-percentile 99; SD: standard deviation; HR: rate of reduction in the level of haemoglobin; PR: rate of reduction in platelet count; NR: rate of reduction in neutrophil count.
Among those patients who presented worsening in haematological parameters after completing treatment with linezolid compared with treatment initiation levels, 6 patients (16%) presented Grade II anaemia, and 3 patients (8%) presented Grade III anaemia. One patient presented Grade I neutropenia, another patient presented Grade 1 thrombocytopenia, and another patient presented Grade III thrombocytopenia.
Two (2) patients (5%) had to discontinue treatment due to thrombocytopenia, and five (5) patients (13.2 %) required blood transfusion during their hospitalization.
No statistically significant differences were observed in the incidence of overall haematological toxicity between patients with and without renal failure (42% vs. 42%, p = 0.970), or between patients with a CrCl above or below 30 mL/min (67% vs. 40%, p = 0.369).
The analysis of the connection between CrCl and the rate of reduction in haemoglobin, platelets and neu-trophils was conducted through linear regression, and did not show statistical significance for any of the relations (R2 = 0.0187, p = 0.4131; R2 = 0.0018, p = 0.7982 and R2 = 0.0168, p = 0.4374, respectively). The correlation between the variables mentioned in the Spearman Correlation Test was not significant either (p = 0.7771, p = 0.4692 and p = 0.9449, respectively).
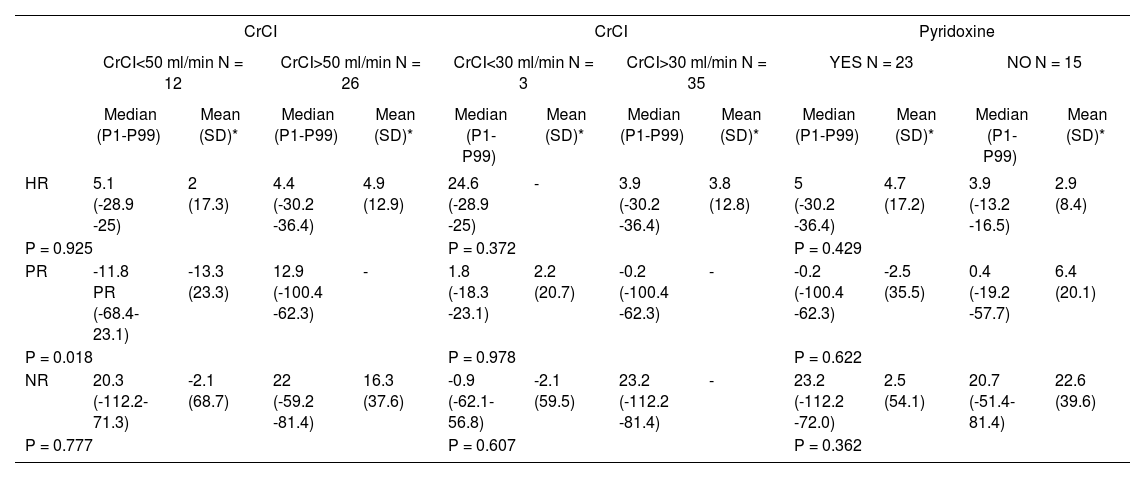
However, statistically significant differences were found in the rate of reduction in platelet count between patients with and without renal failure (p = 0.0185). This result was not repeated with those patients with CrCl below 30 mL/min (p = 0.9784), as appears in table 3, but this could be due to the fact that only 3 patients presented CrCl < 30 ml/min.
Comparison of the rate of reduction in cell count or haemoglobin in patients with and without renal failure and with or withour pyridoxine. Data are presented as median (percentile 1 and percentile 99) and mean (standard deviation)
| CrCI | CrCI | Pyridoxine | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CrCI<50 ml/min N = 12 | CrCI>50 ml/min N = 26 | CrCI<30 ml/min N = 3 | CrCI>30 ml/min N = 35 | YES N = 23 | NO N = 15 | |||||||
| Median (P1-P99) | Mean (SD)* | Median (P1-P99) | Mean (SD)* | Median (P1-P99) | Mean (SD)* | Median (P1-P99) | Mean (SD)* | Median (P1-P99) | Mean (SD)* | Median (P1-P99) | Mean (SD)* | |
| HR | 5.1 (-28.9 -25) | 2 (17.3) | 4.4 (-30.2 -36.4) | 4.9 (12.9) | 24.6 (-28.9 -25) | - | 3.9 (-30.2 -36.4) | 3.8 (12.8) | 5 (-30.2 -36.4) | 4.7 (17.2) | 3.9 (-13.2 -16.5) | 2.9 (8.4) |
| P = 0.925 | P = 0.372 | P = 0.429 | ||||||||||
| PR | -11.8 PR (-68.4-23.1) | -13.3 (23.3) | 12.9 (-100.4 -62.3) | - | 1.8 (-18.3 -23.1) | 2.2 (20.7) | -0.2 (-100.4 -62.3) | - | -0.2 (-100.4 -62.3) | -2.5 (35.5) | 0.4 (-19.2 -57.7) | 6.4 (20.1) |
| P = 0.018 | P = 0.978 | P = 0.622 | ||||||||||
| NR | 20.3 (-112.2-71.3) | -2.1 (68.7) | 22 (-59.2 -81.4) | 16.3 (37.6) | -0.9 (-62.1-56.8) | -2.1 (59.5) | 23.2 (-112.2 -81.4) | - | 23.2 (-112.2 -72.0) | 2.5 (54.1) | 20.7 (-51.4-81.4) | 22.6 (39.6) |
| P = 0.777 | P = 0.607 | P = 0.362 | ||||||||||
CrCI: creatinine clearance estimated through the Cockcroft-Gault Equation; P1-P99: percentile 1 -percentile 99; SD: standard deviation; HR: rate of reduction in the level of haemoglobin; PR: rate of reduction in platelet count; NR: rate of reduction in neutrophil count. N= number of patients; P: probability.
Regarding the impact of pyridoxine, no significant differences were found between the incidence of hae-matological toxicity between patients who received pyri-doxine and those who did not receive it (48% vs, 33%, p = 0.376), and no differences were found in the rate of reduction in haemoglobin, neutrophils or platelets between these two groups of patients (Table 3).
When studying the connection between the duration of treatment with linezolid and the reduction in haemoglobin level and the platelet and neutrophil count, this was not statistically significant: R2 = 0-0442, p = 0.2053, R2 = 0.0031 p = 0.7381 and R2 = 0.0012, p = 0.8366, respectively.
DiscussionIn this study, 42% of those patients treated with li-nezolid presented some type of haematological toxicity, with higher incidence of thrombocytopenia (24%) and neutropenia (21%). Linezolid-induced haematologi-cal toxicity has been described in literature in different studies, as thrombocytopenia in 11 out of 24 patients (46%)8, or in 6 out of 19 patients (32%)7, and anaemia, in 6 out of 24 patients (25%)8. In our case, the incidence of toxicity seems slightly lower than that described, though the small size of the samples in all studies makes it difficult to compare their outcomes. Haematological toxicity led to treatment discontinuation in 5% of patients treated. The cause for treatment discontinuation is not accurately known in some patients, therefore this rate could be slightly superior. In any case, it seems to be lower than that described in literature. In the study by Soriano A et al.9, treatment was discontinued in 7 out of 52 patients (13%) due to severe thrombocytopenia, and in 4 out of 52 patients (8%) due to severe anaemia. Pla-chouras D et al.8 state that they discontinued treatment in 15 of 24 patients (63%) due to adverse effects.
One factor that could contribute to the difference in the incidence of haematological toxicity between studies is the duration of treatment. In our study, the median and mean duration of treatment with linezolid was 7.5 days and 8.4 days, respectively, vs. the median 3.5 weeks in the study by Plachouras et al.8, or > 40 days in the study by Soriano A et al.9. Other authors have also described durations of treatments with linezolid superior to the one in our study, such as mean durations (MD) of 16.9 (10) days15, 12.1 (7.1) days14, and 15.9 weeks (range: 6-36)10. The study by Senneville et al.10 only included patients with chronic osteomyelitis, and Plachouras et al.8 only studied patients with bone and prosthetic joint infections of long evolution. In our study, the majority (65.8%) of patients were diagnosed with a respiratory infection and skin and soft tissue infection. On the other hand, only 5 patients (13.1%) were diagnosed with bone and/or prosthetic joint infection. The duration of treatment with linezolid for respiratory infection and skin and soft tissue infection is usually lower than the duration of treatment in cases of bone and/or prosthetic joint infection18–20.
In our study, no significant association was found between treatment duration and haematological toxicity, possibly due to the short duration of the majority of treatments. However, in literature, different authors have observed an association between both. Gerson et al.21, observed a higher risk of developing thrombocytopenia and anaemia in those patients on treatment with line-zolid for more than 2 weeks. On the other hand, Attassi et al.7 associated thrombocytopenia with treatments of over 10 days of duration. Senseville et al.10 had evidence of anaemia in therapies of over 4 weeks of duration in patients with chronic osteomyelitis.
In the study conducted in our centre, 13% of those patients with bone marrow toxicity required blood transfusion during hospitalization; this is lower than what has been described in bibliography. In the study by Senseville et al.10, 28.9% of patients required a blood transfusion; and in the study by Attasi et al.7, 21% of patients required platelet transfusion. This discrepancy could be due, once again, to the shorter duration of treatment with linezolid in our patients.
Regarding the influence of renal function in the development of haematological toxicity, no significant connection between them was observed in our study, except for the fact that patients with RF did present a significantly higher reduction in platelets. In this regard, it is worth pointing out that in patients with normal renal function or mild to moderate renal failure, linezolid is mostly excreted in urine as hydroxyethylglycine (40%), unaltered drug (30%), and aminoethoxy acetic acid (10%). Extra-renal clearance represents approximately 65% of the total clearance for linezolid1,2. Therefore, initially, these patients should not present a clinically significant higher exposure to linezolid, or develop haema-tological toxicity with higher frequency.
There is little evidence about the connection between renal function and linezolid pharmacokinetics. However, certain authors such as Soriano et al.9 have reached the conclusion that the risk of toxicity caused by the drug is superior in those patients with renal failure. Sasaki et al.12 concluded that dosing adjustment should be considered for those patients with CrCl < 30 mlVmin and associated liver cirrhosis. In agreement with our results, Lin et al.15 observed a higher incidence of thrombocyto-penia in those patients with renal failure. They observed a higher incidence of thrombocytopenia in patients with prolonged treatments for over 2 weeks and renal failure; they have also identified the previous administration of vancomycin as a risk factor.
Regarding the use of pyridoxine with the aim to prevent linezolid-induced haematological toxicity, no protective effect was observed in this study. The use of pyridoxine with this objective is currently a widespread practice. However, the evidence available does not provide conclusive data supporting any benefit in its administration. Youssef et al.11 observed that the administration of pyridoxine at a 50mg daily dose could have some impact on the prevention of linezolid-induced anaemia, but not in terms of thrombocytopenia or leukopenia. On the contrary, Plachouras et al.8 and Soriano et al.9, did not find any significant differences in the prevention of linezolid-induced myelosuppression, when said vitamin was added on to treatment. Therefore, it seems necessary to conduct more studies with larger sample sizes in order to evaluate adequately its potential impact.
This study presents the advantage of reflecting the usual clinical practice in many hospitals; however, it also has some limitations. Its main limitations are the reduced sample size and its retrospective nature. Therefore, the results obtained should be confirmed through prospective studies on a larger number of patients. On the other hand, the mean duration of treatment has been lower than that described in literature, and this fact could have influenced the outcomes.
In conclusion, there is a high incidence, of around 42%, of haematological toxicity in patients treated with linezolid in clinical practice, in some cases with severe consequences, which can lead to treatment interruption. Therefore, it is particularly relevant to conduct a monitoring of haematological parameters both at treatment initiation and during the course of treatment with linezolid. The impact of renal failure on its development is not clear, and should be confirmed through studies of a larger scale. The use of pyridoxine for its prevention is not clear either, and haematological monitoring is necessary regardless of its use.

