

pH is a critical factor for all those medications prepared as aqueous liquid forms, because it has an impact on the solubility of the molecule, determining the stability of medications, the biological tolerability of the formulation, and the activity of the molecule. The objective of this study is to determine the optimum pH range for the oral liquid formulations more frequently prepared at the Pharmacy Unit, in order to standardize and incorporate said value into the standard protocols of action as a quality control criterion.
MethodThe study was conducted in three stages. The first stage consisted in a retrospective study of the records of preparation of those oral liquid formulations prepared at least 5 times since January, 2015 to December, 2016, in our Pharmacy Unit; the main value and standard deviation of the pH values recorded for each formulation were calculated. In a second stage, there was a bibliographic search in order to understand the pH for the maximum stability of the molecule, and to confirm if this characteristic was recorded as a requirement for quality control in the procedures described in the formulation guidelines. In the third stage, it was confirmed if the pH values determined coincided with the maximum stability pH described in literature, and acceptance ranges were established.
ResultsIn total, 31 formulations were reviewed (14 solutions / 17 suspensions). The maximum stability pH value was known for 19 (61.3%) of the molecules and/or oral liquid formulations evaluated; 15 (78.9%) of these were within this range, and the remaining 4 (21.1%) presented a standard deviation of ± 0.5 regarding the pH value referenced in the bibliography. The pH range for the same standard work procedure ranged between 0.32 and 1.51. An acceptance pH range of ± 0.75 was determined as quality control.
ConclusionsAn optimal pH range has been determined for the 31 oral liquid formulations more widely prescribed in our hospital. This characteristic should be part of the galenic validation for these preparations, as well as of its routine quality control, in order to ensure their quality and efficacy.
El pH es un factor crítico para todos aquellos medicamentos que se encuentran en formas líquidas acuosas, ya que puede ejercer un efecto sobre la solubilidad del principio activo condicionando la estabilidad de los medicamentos, la tolerancia biológica de la forma farmacéutica y la actividad del principio activo. El objetivo de este trabajo es establecer el rango óptimo de pH de las fórmulas orales líquidas más frecuentemente elaboradas en el Servicio de Farmacia para estandarizar e incorporar dicho valor en los protocolos normalizados de trabajo como criterio de control de calidad.
MétodoEl estudio se desarrolló en tres fases. En una primera fase se realizó un estudio retrospectivo de los registros de elaboración de las fórmulas orales líquidas elaboradas, al menos 5 veces, desde enero de 2015 a diciembre de 2016 en nuestro Servicio de Farmacia, y se calculó el valor medio y la desviación estándar de los valores de pH registrados para cada fórmula. En una segunda fase se realizó una búsqueda bibliográfica para conocer el pH de máxima estabilidad del principio activo y comprobar si esta característica se registra como requisito de control de calidad en los procedimientos descritos en los formularios de referencia. En una tercera fase se comprobó si los pH determinados se correspondían con el de máxima estabilidad descrito en la literatura y se establecieron rangos de aceptación.
ResultadosSe revisaron un total de 31 fórmulas (14 soluciones/17 suspensiones). Se conocía el valor del pH de máxima estabilidad de 19 (61,3%) de los principios activos y/o fórmulas orales líquidas evaluadas, de las cuales 15 (78,9%) se encontraban dentro del mismo y las 4 restantes (21,1%) presentaron una desviación estándar de ± 0,5 con respecto al valor de pH referenciado en la bibliografía. El rango de pH para un mismo procedimiento normalizado de trabajo oscilaba entre 0,32 y 1,51. Se estableció como control de calidad un rango de aceptación de pH de ± 0,75.
ConclusionesSe ha establecido un rango óptimo de pH para las 31 fórmulas orales líquidas de mayor prescripción en nuestro hospital. Esta característica debería formar parte de la validación galénica de estas preparaciones, así como de su control de calidad rutinario, para asegurar la calidad y eficacia de las mismas.
The pH of an aqueous solution is a critical factor to be considered for all those medications prepared in aqueous liquid forms. The potential effect of pH on solubility will be a decisive factor for the stability of the medications to be administered. Moreover, the biological tolerability of the formulation can be compromised, as well as the activity of the active principle (AP)1.
The solubility of acid and basic drugs is pH-dependent, and based on its ionization constant, which creates a balance between the ionized and non-ionized species, and leads to the dilution of the acid and/or the base. Aqueous reactions are generally catalyzed by pH. There have been studies measuring the degradation rates at different pH values, keeping constant the temperature, ionic strength, and concentration of the solvent. The conclusion of these studies was that, if pH is not within a maximum stability range, the non-ionized form of the drug will prevail, leading to the creation of insoluble precipitates2.
Each AP has a pH range for its maximum stability, and it can lose activity outside this range, due to physical and chemical transformations. The combination with diluents, excipients, and other medications with a different pH, can trigger undesired effects and compromise the stability of the formulation. It has been confirmed that, for example, folic acid and furosemide will precipitate at a pH below 8 and 7, respectively; omeprazole is degraded at pH values below 7.8; propranolol breaks down if exposed to alkaline pH values, and captopril experiences oxidative degradation in means presenting pH values above 43.
Therefore, pH determination is important for the preparation of oral liquid formulations (OLFs), because it affects the solubility, activity, absorption, biological tolerability and stability of the AP4,5.
However, most formulation guidelines with acknowledged prestige about OLFs for pediatric patients, such as: “Formulación Pediátrica Manuela Atienza”, “Standardised formulations for New Zealand”, “Nationwide Children's Hospital”, “Hospital for Sick Children” and “University of Michigan College of Pharmacy”, do not include any pH values for maximum stability of the preparations described. On the other hand, the Spanish National Formulary (FNE) includes in its procedure No. PN/L/CP7001/00 the determination of pH as quality control for solutions, suspensions and syrups, but exclusively for formulations prepared in lots6–11.
Given the lack of compatibility data between OLF components, we hereby state that knowing the pH values for maximum stability of the medications to be administered is a predictive factor that can prevent serious stability problems, and that its determination will ensure the quality and efficacy of the formulations prepared.
The objective of this study is to determine the optimal pH range for the OLFs more frequently prepared at the Hospital Pharmacy Unit (HPU), in order to standardize and incorporate said value into the standard work procedures (SWPs) as a quality control criterion.
Methods- 1.
A retrospective study was conducted on the preparation records of all OLFS prepared at the HPU from January, 2015 to December, 2016. Those OLFS prepared with a ≥ 5 frequency were selected, and the pH values evaluated were collected. Mean value and standard deviation were calculated for each preparation, as well as the range, obtained through the difference between the maximum and minimum values recorded. These pH determinations were conducted with a sensIONTM pH31 meter®.
- 2.
In order to determine the maximum stability pH of the AP, the following bibliographic sources were reviewed: the product specifications of the molecules by our main provider (www.acofarma.com/es/formulación-magistral/fichas-tecnicas) and the books: Trissel's “Stability of Compounded Formulations” 2nd edition, and “Handbook of Extemporaneous Preparation” (2010), as well as the product specifications by the Spanish Agency of Medicines and Medical Devices (AEMPS) for branded medications to be administered intravenously as solution, and the United States Pharmacopeia 32th edition and National Formulary 27th edition (USP 32- NF 27)12–16.
The most relevant pediatric formulation guidelines previously mentioned were also consulted6–10.
- 3.
Finally, the pH values recorded were compared with the maximum stability values stated in the bibliography, and an acceptance range was determined for each of the OLFs evaluated.
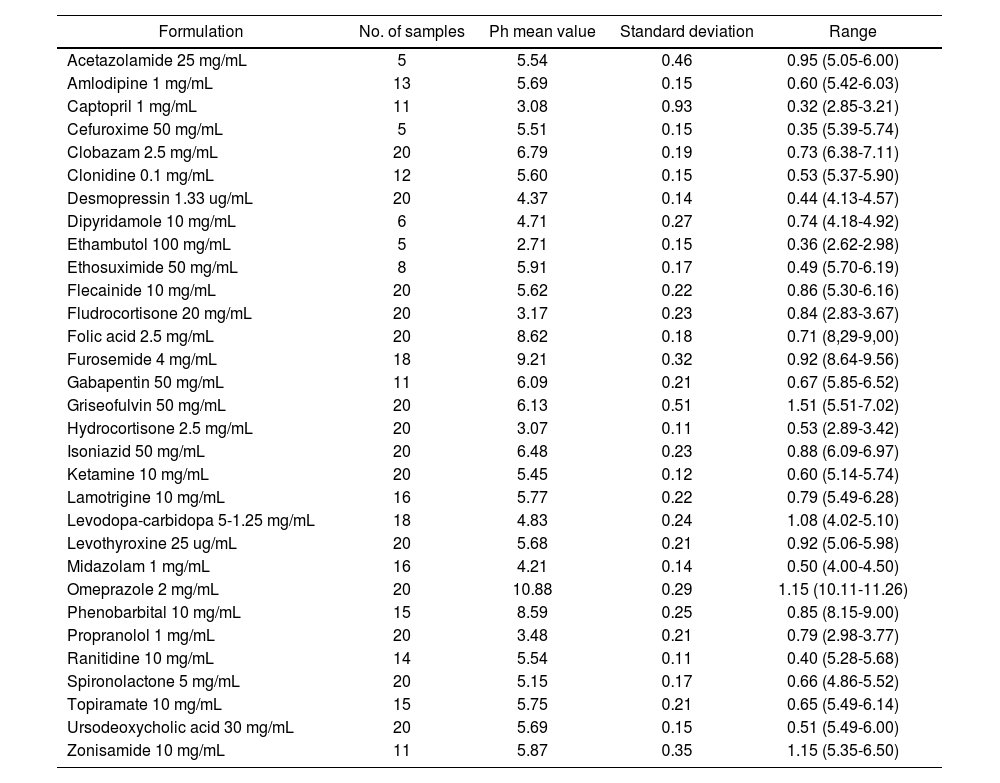
In total, 31 OLFs were reviewed according to the criteria of the first stage of the study: 14 solutions and 17 suspensions (Table 1). For all OLFs prepared during the period of the study, and which met the inclusion criteria, the following data were collected: pH mean value, standard deviation, and pH ranges for the same SWP (Table 2). The latter value ranged between 0.32 and 1.51.
Formulation and composition of the OLFs prepared at the HPU
| PREPARATION | FORMULATION | COMPOSITION | |
|---|---|---|---|
| Acetazolamide 25 mg/mL | Suspension |
|
|
| Amlodipine 1 mg/mL | Suspension |
|
|
| Captopril 1 mg/mL | Solution |
|
|
| Cefuroxime 50 mg/mL | Suspension |
|
|
| Clobazam 2.5 mg/mL | Suspension |
|
|
| Clonidine 0.1 mg/mL | Suspension |
|
|
| Desmopressin 1.33 μg/mL | Solution |
|
|
| Dipyridamole 10 mg/mL | Suspension |
|
|
| Ethambutol 100 mg/mL | Solution |
|
|
| Ethosuximide 50 mg/mL | Solution |
|
|
| Flecainide 10 mg/mL | Solution |
|
|
| Fludrocortisone 20 μg/mL | Suspension |
|
|
| Folic acid 2.5 mg/mL | Solution |
|
|
| Furosemide 4 mg/mL | Solution |
|
|
| Gabapentin 50 mg/mL | Solution |
|
|
| Griseofulvin 50 mg/mL | Suspension |
|
|
| Hydrocortisone 2.5 mg/mL | Suspension |
|
|
| Isoniazid 50 mg/mL | Solution |
|
|
| Ketamine 10 mg/mL | Solution |
|
|
| Lamotrigine 10 mg/mL | Suspension |
|
|
| Levodopa-Carbidopa 5-1.25 mg/mL | Suspension |
|
|
| Levothyroxine 25 μg/mL | Suspension |
|
|
| Midazolam 1 mg/mL | Solution |
|
|
| Omeprazole 2 mg/mL | Solution |
|
|
| Phenobarbital 10 mg/mL | Suspension |
|
|
| Propranolol 1 mg/mL | Solution |
|
|
| Ranitidine 10 mg/mL | Solution |
|
|
| Spironolactone 5 mg/mL | Suspension |
|
|
| Topiramate 10 mg/mL | Suspension |
|
|
| Ursodeoxycholic acid 30 mg/mL | Suspension |
|
|
| Zonisamide 10 mg/mL | Suspension |
|
|
amp: ampoules; caps: capsules; q.s. for: quantity sufficient for; q.s.: quantity sufficient.
pH mean value, standard deviation and range for each compound preparation
| Formulation | No. of samples | Ph mean value | Standard deviation | Range |
|---|---|---|---|---|
| Acetazolamide 25 mg/mL | 5 | 5.54 | 0.46 | 0.95 (5.05-6.00) |
| Amlodipine 1 mg/mL | 13 | 5.69 | 0.15 | 0.60 (5.42-6.03) |
| Captopril 1 mg/mL | 11 | 3.08 | 0.93 | 0.32 (2.85-3.21) |
| Cefuroxime 50 mg/mL | 5 | 5.51 | 0.15 | 0.35 (5.39-5.74) |
| Clobazam 2.5 mg/mL | 20 | 6.79 | 0.19 | 0.73 (6.38-7.11) |
| Clonidine 0.1 mg/mL | 12 | 5.60 | 0.15 | 0.53 (5.37-5.90) |
| Desmopressin 1.33 ug/mL | 20 | 4.37 | 0.14 | 0.44 (4.13-4.57) |
| Dipyridamole 10 mg/mL | 6 | 4.71 | 0.27 | 0.74 (4.18-4.92) |
| Ethambutol 100 mg/mL | 5 | 2.71 | 0.15 | 0.36 (2.62-2.98) |
| Ethosuximide 50 mg/mL | 8 | 5.91 | 0.17 | 0.49 (5.70-6.19) |
| Flecainide 10 mg/mL | 20 | 5.62 | 0.22 | 0.86 (5.30-6.16) |
| Fludrocortisone 20 mg/mL | 20 | 3.17 | 0.23 | 0.84 (2.83-3.67) |
| Folic acid 2.5 mg/mL | 20 | 8.62 | 0.18 | 0.71 (8,29-9,00) |
| Furosemide 4 mg/mL | 18 | 9.21 | 0.32 | 0.92 (8.64-9.56) |
| Gabapentin 50 mg/mL | 11 | 6.09 | 0.21 | 0.67 (5.85-6.52) |
| Griseofulvin 50 mg/mL | 20 | 6.13 | 0.51 | 1.51 (5.51-7.02) |
| Hydrocortisone 2.5 mg/mL | 20 | 3.07 | 0.11 | 0.53 (2.89-3.42) |
| Isoniazid 50 mg/mL | 20 | 6.48 | 0.23 | 0.88 (6.09-6.97) |
| Ketamine 10 mg/mL | 20 | 5.45 | 0.12 | 0.60 (5.14-5.74) |
| Lamotrigine 10 mg/mL | 16 | 5.77 | 0.22 | 0.79 (5.49-6.28) |
| Levodopa-carbidopa 5-1.25 mg/mL | 18 | 4.83 | 0.24 | 1.08 (4.02-5.10) |
| Levothyroxine 25 ug/mL | 20 | 5.68 | 0.21 | 0.92 (5.06-5.98) |
| Midazolam 1 mg/mL | 16 | 4.21 | 0.14 | 0.50 (4.00-4.50) |
| Omeprazole 2 mg/mL | 20 | 10.88 | 0.29 | 1.15 (10.11-11.26) |
| Phenobarbital 10 mg/mL | 15 | 8.59 | 0.25 | 0.85 (8.15-9.00) |
| Propranolol 1 mg/mL | 20 | 3.48 | 0.21 | 0.79 (2.98-3.77) |
| Ranitidine 10 mg/mL | 14 | 5.54 | 0.11 | 0.40 (5.28-5.68) |
| Spironolactone 5 mg/mL | 20 | 5.15 | 0.17 | 0.66 (4.86-5.52) |
| Topiramate 10 mg/mL | 15 | 5.75 | 0.21 | 0.65 (5.49-6.14) |
| Ursodeoxycholic acid 30 mg/mL | 20 | 5.69 | 0.15 | 0.51 (5.49-6.00) |
| Zonisamide 10 mg/mL | 11 | 5.87 | 0.35 | 1.15 (5.35-6.50) |
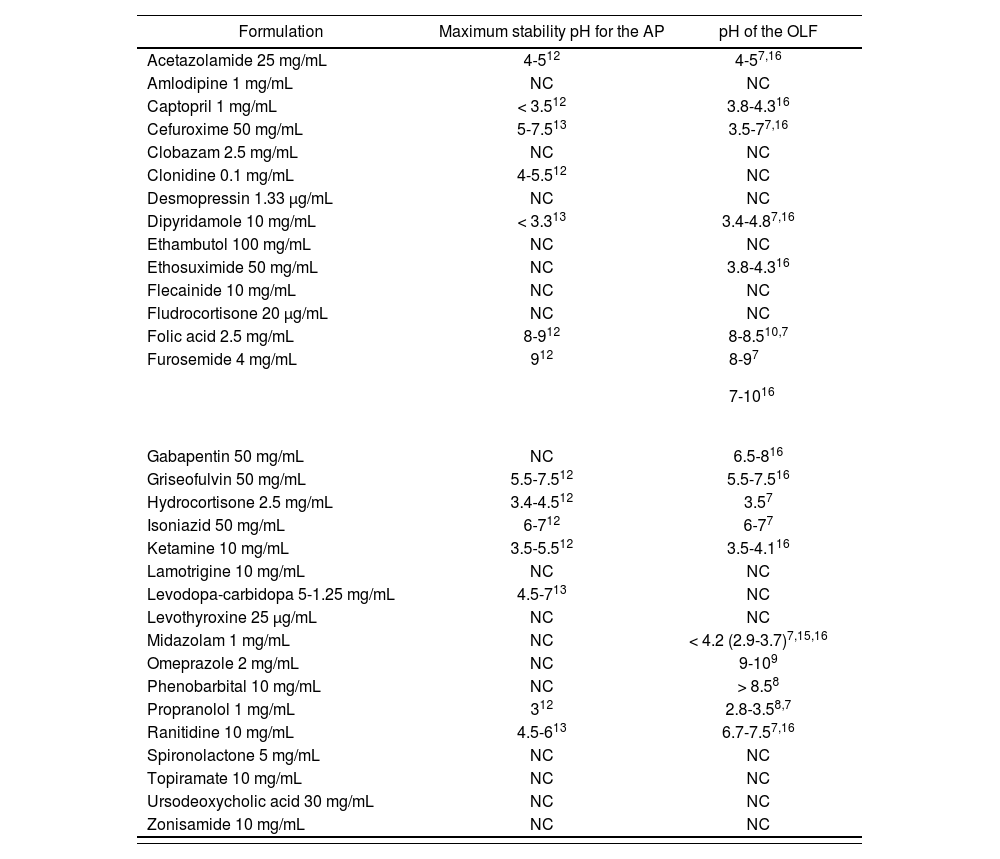
After consulting the different bibliographical sources in order to find the maximum stability pH of the AP, only the value of the 19 (61.3 %) of the APs and/or OLFs evaluated was available.
Regarding the formulation guidelines consulted, a pH value as quality control was determined for 3 (9.7%) of the OLFs selected in the “Formulación Pediátrica Manuela Atienza”; 10 (32.3%), in the “Standardised formulations for New Zealand”, 1 (3.2%) in the “Nationwide Children's Hospital”, 1 (3.2%) in the “University of Michigan College of Pharmacy”, and none in the “Hospital for Sick Children”.
The data on maximum stability pH for APs and OLFs referenced in the bibliography selected appear in tTable 3.
Maximum stability pH values for the active principle and pH values of the oral liquid formulations described in the bibliography reviewed
| Formulation | Maximum stability pH for the AP | pH of the OLF |
|---|---|---|
| Acetazolamide 25 mg/mL | 4-512 | 4-57,16 |
| Amlodipine 1 mg/mL | NC | NC |
| Captopril 1 mg/mL | < 3.512 | 3.8-4.316 |
| Cefuroxime 50 mg/mL | 5-7.513 | 3.5-77,16 |
| Clobazam 2.5 mg/mL | NC | NC |
| Clonidine 0.1 mg/mL | 4-5.512 | NC |
| Desmopressin 1.33 μg/mL | NC | NC |
| Dipyridamole 10 mg/mL | < 3.313 | 3.4-4.87,16 |
| Ethambutol 100 mg/mL | NC | NC |
| Ethosuximide 50 mg/mL | NC | 3.8-4.316 |
| Flecainide 10 mg/mL | NC | NC |
| Fludrocortisone 20 μg/mL | NC | NC |
| Folic acid 2.5 mg/mL | 8-912 | 8-8.510,7 |
| Furosemide 4 mg/mL | 912 | |
| Gabapentin 50 mg/mL | NC | 6.5-816 |
| Griseofulvin 50 mg/mL | 5.5-7.512 | 5.5-7.516 |
| Hydrocortisone 2.5 mg/mL | 3.4-4.512 | 3.57 |
| Isoniazid 50 mg/mL | 6-712 | 6-77 |
| Ketamine 10 mg/mL | 3.5-5.512 | 3.5-4.116 |
| Lamotrigine 10 mg/mL | NC | NC |
| Levodopa-carbidopa 5-1.25 mg/mL | 4.5-713 | NC |
| Levothyroxine 25 μg/mL | NC | NC |
| Midazolam 1 mg/mL | NC | < 4.2 (2.9-3.7)7,15,16 |
| Omeprazole 2 mg/mL | NC | 9-109 |
| Phenobarbital 10 mg/mL | NC | > 8.58 |
| Propranolol 1 mg/mL | 312 | 2.8-3.58,7 |
| Ranitidine 10 mg/mL | 4.5-613 | 6.7-7.57,16 |
| Spironolactone 5 mg/mL | NC | NC |
| Topiramate 10 mg/mL | NC | NC |
| Ursodeoxycholic acid 30 mg/mL | NC | NC |
| Zonisamide 10 mg/mL | NC | NC |
AP: active principle; OLFs: oral liquid formulations; UNKN: unknown.
Of those 19 OLFs and/or PAs with a known pH range for maximum stability, 15 (78.9%) were within said range, and the remaining 4 (21.1%) presented a ± 0.5.standard deviation.
Based on the data collected in the bibliography consulted, and the variability of the determinations evaluated, it was determined to include pH as regular quality control for SWPs with a ± 0.75 acceptance range.
DiscussionThe pH is one of the factors with higher impact on the stability of a formulation in aqueous solution. Knowing the maximum stability pH for an AP of OFLs is essential to guarantee the quality of the preparation; it must remain stable during all the validity and preservation period established1.
In most of the formulation guidelines reviewed, pH is not included either as a control to be conducted or an acceptance range; a pH range for each monograph is only described in USP 32- NF 27. In the FNE, pH determination (PN/L/CP/001/00) is included as a product control procedure, and it is compulsory for all solutions, suspensions, syrups and gels prepared in lots11,16.
It is worth highlighting that there is limited bibliography providing data on the pH values for maximum stability of an AP and/or OLF.
Given that there are many medications, such as furosemide, propranolol, omeprazole and captopril, with an already known and well defined pH for maximum stability, and the formulation is not stable unless within it, we consider that this is a value that must be known and evaluated, even for individualized formulations not prepared in lots 5. The SWP established should include this criterion.
For those OLFs with unknown maximum stability pH range, or insoluble AP, pH determination is still a quality indicator, because it must stay stable and reproducible for the same SWP, as has been demonstrated in the study.
Even though the HPU evaluated and recorded pH routinely for all individual OLFs, there was no acceptance range established for each SWP. This study has been useful in order to include this criterion in the protocol, and its evaluation as quality control.
Knowing the maximum stability pH in the preparation of an OLF, and determining an acceptance range as quality control, are indispensable requirements for an adequate galenic validation, and to guarantee treatment efficacy.
FundingNo funding.
Conflict of interestsNo conflict of interests.
Contribution to scientific literature.
The majority of pediatric formulation guidelines do not include pH determination as quality control for the preparation of oral liquid formulations.
The bibliographic search conducted in this study shows the impact of pH in the stability of these preparations, and the importance of knowing the pH range for maximum stability of the molecule. Being able to determine said value as quality control will allow us to guarantee the reproducibility of the same standard work procedure, and a correct galenic validation of the formulation prepared.

