
Despite the global stabilization of the number of new HIV infections in recent years, there has been an increase in new infections among men who have sex with men. This fact indicates the lack of effectiveness of the measures and prevention campaigns established so far for this group. It is therefore necessary to implement alternative preventive measures for them. Pre-exposure pharmacological prophylaxis (PrEP) is one of the best evaluated options and has had high protection rates in both clinical and real-life trials. The strategy has also shown an adequate profile in terms of safety, tolerance, adverse effects and cost-effectiveness in the studies carried out to assess this important topic.
En los últimos años se ha objetivado un incremento de las nuevas infecciones por el VIH en el grupo de hombres que tienen sexo con hombres, lo que indica la ausencia de eficacia de las campañas y medidas preventivas instauradas en dicho grupo.
Es necesario, por tanto, implementar medidas preventivas alternativas, siendo la profilaxis farmacológica pre-exposición (PrEP) una de las opciones mejor evaluadas tanto en ensayos clínicos como en la vida real, habiéndose demostrado tasas de protección superiores al 80% cuando se administra en los casos indicados y con buen cumplimiento terapeútico.
La estrategia ha demostrado, además, un perfil adecuado en seguridad, tolerancia y efectos adversos, siendo además coste-efectiva según los estudios realizados para valorar este importante aspecto.
According to the latest data presented regarding the number of new HIV infections in >13-year-old patients, there has been a reduction in its overall incidence in the United States in the period from 2008 to 2014. However, when analyzing the different populations at risk of infection, it has been observed that there is an increase in new infections in the group of men who have sex with men (MSM) with ages between 25 and 34 years, as well as in those >55-year-old1.
In Spain, according to data by the Ministry of Health, 3,366 new cases of HIV infection were reported during 2014. After an estimation taking into account the current delay in the report of cases, it is calculated that in 2014 there were 9.34 new infections per 100,000 inhabitants, and 54% of them were in MSM. This represents an increase from previous years in the group of MSM population between 20 and 30 years of age2.
This increase in new infections in the MSM group within a context of overall stability, and even reduction in new cases during recent years, represents an indication of the lack of efficacy of prevention measures and campaigns implemented so far in said group. Therefore, it is necessary to implement alternative preventive measures; one of the better valued options is Pre-Exposure Pharmacological Prophylaxis (PrEP). It must be highlighted that clinical trial outcomes have been replicated consistently in some of the places where it has been widely used in cases within the indication.
Drug administration in order to prevent an infection or its clinical consequences is an already well-known strategy, and it has been applied in different medical scenarios, such as prevention of malaria by the administration of antimalarial treatment, or antibiotic administration as surgical prophylaxis. Similarly, the theoretical basis of PrEP consists in the administration of antiretrovirals before the sexual contact that could transmit the HIV infection.
In this article, we will briefly review the main aspects of this strategy, with particular focus on its efficacy and safety.
Studies on prep efficacy as a prevention strategy for HIV infectionThe first study which demonstrated the efficacy of oral PrEP as prevention strategy against HIV was the iPrex study, published in 20103. This study included 2,499 MSM subjects who were HIV-negative, or transgender women (TGW) who had sexual relationships with men. All of them were randomized to receive a combination of emtricitabine and tenofovir disoproxil fumarate (FTC/TDF) or placebo once a day. After one year of follow-up, 36 persons in the FTC-TDF group had become infected by HIV, vs. 64 in the placebo group, with a 44% reduction rate of new infections (CI95% 15-63) in the PrEP arm compared with placebo.
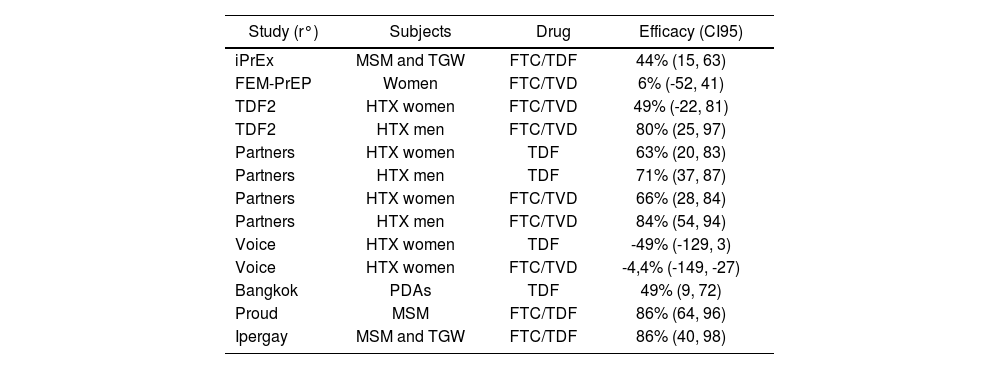
Further studies have been conducted after the first one, which have contributed with more and better data on the efficacy of this prevention strategy. We will discuss their most relevant aspects; there is also a summary of these data in Table 1.
Main clinical trials published on PrEP
| Study (r°) | Subjects | Drug | Efficacy (CI95) |
|---|---|---|---|
| iPrEx | MSM and TGW | FTC/TDF | 44% (15, 63) |
| FEM-PrEP | Women | FTC/TVD | 6% (-52, 41) |
| TDF2 | HTX women | FTC/TVD | 49% (-22, 81) |
| TDF2 | HTX men | FTC/TVD | 80% (25, 97) |
| Partners | HTX women | TDF | 63% (20, 83) |
| Partners | HTX men | TDF | 71% (37, 87) |
| Partners | HTX women | FTC/TVD | 66% (28, 84) |
| Partners | HTX men | FTC/TVD | 84% (54, 94) |
| Voice | HTX women | TDF | -49% (-129, 3) |
| Voice | HTX women | FTC/TVD | -4,4% (-149, -27) |
| Bangkok | PDAs | TDF | 49% (9, 72) |
| Proud | MSM | FTC/TDF | 86% (64, 96) |
| Ipergay | MSM and TGW | FTC/TDF | 86% (40, 98) |
Another significant study was the TDF2, sponsored by the Centres for Disease Control and Prevention (CDC) in Atlanta. This study analyzed the use of FTC/TDF or placebo in HIV-negative men and women in Botswana with high-risk sexual behaviour4. During follow-up, there were 9 infections in the treatment arm (1.2 infections/100 person-years of follow-up (pyf) vs. 24 in the placebo arm (3.1 infections/100 pyf; which shows a 62-2% efficacy of the PrEP in this study (CI95%: 21.5-83.4).
The Partners study, conducted in Kenya and Uganda, included 4,757 serodiscordant heterosexual couples, who were randomized to receive TDF only, FTC/TDF in combination, or placebo5. During the 23 months of followup, there were 82 HIV infections: 17 in the TDF arm (0.65 instances/100 person-years of follow-up), 13 in the FTC/TDF arm (0.50/100 person-years of follow-up) and 52 in the placebo group (1.99/100 person-years of follow-up). Therefore, the use of TDF offered a 67% protection compared with the placebo arm (CI95% 44-81), and there was a 75% protection for the FTC/TDF arm (CI95% 55-87).
Since 2015, data from the studies conducted in Europe have also been reported. Of the two most important, the first was the PROUD study6, which included 544 MSM randomized to receive 1 daily FTC/TDF immediately, or to delay treatment initiation by 12 months. All participants received training on how to reduce risk during sexual relationships, and condoms were provided throughout the study. During follow-up, both arms presented a high incidence of STIs, without statistical differences between them. The study was interrupted by the Safety Committee, when it was confirmed that those persons with a delayed treatment initiation had a higher risk of HIV infection than those receiving immediate treatment. There were 3 infections in the immediate treatment arm, vs. 20 in the delayed group (9.0/100 persons-year), and with an 86% reduction (CI90% 64-96). According to these data, it would be necessary to initiate prophylaxis in 13 persons in order to prevent one new HIV infection. Of the three persons who were infected in the immediate treatment arm, one had entered the study with an existing infection (HIV-negative but positive HIV-PCR at baseline): while the other two had stopped taking prophylaxis some time before the infection.
The second study is the Ipergay, conducted in France and Canada, which included 400 MSM or transgender women (TGW) not infected by HIV and at high risk of infection7. After inclusion, they were randomized to receive prophylaxis with FTC/TDF or placebo. In this case, prophylaxis was on demand with the administration of 2 FTC/TDF tablets between 2 and 24 hours before having a sexual relationship, followed by 1 tablet at 24 hours, and another tablet at 48 hours after said relationship. In case that they continued having sexual relationships, they continued receiving 1 daily tablet until 48 hours after the last intercourse. If there were any subsequent sexual relationships, prophylaxis was initiated again, with 2 FTC/TDF tablets followed by 1 daily tablet until 48 hours after the last intercourse. The control arm received the same regimen, but with placebo. Just as in the PROUD study, all participants received training in order to minimize risk during intercourse, and condoms were provided throughout follow-up. Again, there was a high incidence of STIs during follow-up, which confirms high-risk relationships in both arms of the study. The same as in the PROUD study, the Safety Committee interrupted this study 9 months after its initiation, because there were 2 HIV infections during follow-up in the study arm (0.91 infections/100 person-years) vs. 14 in the placebo arm (6.6/100 personyears). Prophylaxis had an 86% efficacy (CI95% 40-98, p=0.002), and it was necessary to treat 18 persons in order to prevent 1 new infection. Again, none of the two persons infected in the FTC/TDF group had detectable TAF levels in blood.
The HPTN 067 / ADAPT study (Alternative Dosing to Augment PrEP PillTaking) is a Phase II clinical trial designed to confirm if non-daily PrEP dosing regimes could make compliance easier8. The study was conducted on 3 different populations: MSM in Bangkok, MSM in Harlem, and heterosexual women in Cape Town. In the three arms, participants were randomized to receive 1 daily TDF/FTC tablet, or a non-daily tablet based on time (1 tablet twice a week plus 1 extra tablet after each sexual contact), or based on sexual activity (1 tablet before and 1 tablet after each sexual contact). In the three sub-groups, daily prophylaxis achieved better rates in the reduction of new infections, also demonstrating better treatment adherence. Overall, the Harlem cohort achieved the worst response (65% for the Harlem cohort, 85% for the Bangkok cohort, 75% for the Cape Town cohort).
Against these studies which have demonstrated the efficacy of PrEP, other studies have been reported where this efficacy has been questioned. The FEM-Prep study included 2,120 HIV-negative women in Kenya, South Africa and Tanzania, who were randomized to FTC/TDF or placebo9. In total, 33 women were infected in the FTC/TAF group (incidence of 4.7 infections/100 person-years of follow-up [pyf]) vs. 35 in the placebo arm (5 infections/100 pyf), with a 0.94 HR of protection (CI95% 0.59-1.52). The Voice study, conducted in South Africa, Zimbabwe and Uganda, included 5,029 HIV-negative women who were randomized to TDF only, FTC/TDF, 1% vaginal TDF gel, and two placebo arms, one on oral treatment and the other one on vaginal gel10. In total, there were 312 infections with a 5.7/100 pyf incidence. In this instance, none of the 3 study arms offered protection vs. placebo. The efficacy of TDF administered as monotherapy was of -49%, FTC/TDF reached a -4.4% efficacy, and finally, the vaginal gel showed a 14.5% efficacy, in this last case without any statistical significance.
Outside sexual transmission, a study conducted in Bangkok showed a 48.9% level of protection (CI95% 9.6-72.2), among 2,413 parenteral-drug addicts (PDAs) who were not infected with HIV, and who were randomized to receive TDF or to the control arm11.
In the majority of cases, the differences in PrEP efficacy between the different studies lie in their different treatment compliance. For example, in the VOICE study, were the efficacy of PrEP was not demonstrated, TDF levels were only detected in 30%, 29% and 25% of the patients randomized to receive TDF, FTC/TDF or TDF gel10. Likewise, only 28% of women assigned to the FTC/TDF arm had detectable FTC levels in the FEM-PrEP study9. In a sub-analysis of the iPrex study, when analyzing those persons randomized to receive FTC/TDF who were infected by HIV vs. those without the infection, the former presented lower TDF levels, both in the seroconversion visit (8% vs. 44%, p<0.001), and in the visit 90 days before (11% vs. 51%, p<0.001)9. In fact, a 90% reduction was demonstrated in the risk of HIV infection in those who presented detectable TDF concentrations in peripheral blood cells.
Similar data were found in the PARTNERS study; in this case, only 21% of the infected persons had levels considered as protective (>40 ng/mL) vs. 71% in non-infected persons5. Even in those persons who exceeded said concentration, there was an 88% efficacy of prophylaxis (CI95% 60-96) for those who received TDF and 91% (CI95% 47-98) for those who received FTC/TDF.
Finally, in the study conducted in Bangkok among PDAs, the efficacy reached 73.5% (CI95% 16.6-94) when the analysis was restricted to persons with good treatment compliance, and with detectable TDG levels11.
Besides low treatment adherence as a clear cause for PrEP failure, some studies might indicate that some pharmacological differences coulf also explain these discrepancies. For example, after PrEP administration, it has been confirmed that TDF levels in male rectal tissue are between 10 and 100 times higher than those reached in female cervico-vaginal tissue; this could point towards a worse efficacy of PrEP among women12.
Real-life data on PrEPAfter the first published clinical trials, in 2012 the FDA approved the use of PrEP, and in 2014 the CDC issued some recommendations for its use13. Currently, many studies have been reported about its use in real life, and under these circumstances it does not seem that results will deviate too far from clinical trial reports. In data reported within the San Francisco area by the Kaiser Permanente Insurance Company, between July, 2012 and February, 2015, after PrEP was prescribed to 657 persons with a follow-up of 388 persons/year, and even though there was a high rate of TSI diagnosis (28% of these persons presented at least one TSI during follow-up), there were no cases of HIV infection14.
In the DEMO Project study, conducted in San Francisco and Miami clinics, PrEP was administered to 557 MSM and TGW between October, 2012 and January, 201415. In total, there were 5 HIV infections; three of them were considered primary infections existing at the time of inclusion, and only 1 appeared during follow-up (0.43/100 pyf incidence). Once more, none of these two last participants had protective levels of TDF in their blood at the time of infection.
It is worth highlighting the ATN 110 study, which analyzed the use of PrEP in a population of 200 18-to-22-year old MSM16. In total, there were 4 cases of HIV infection (3.29/100 pyf). In one of them, it was demonstrated that the patient was already infected with HIV at the time of inclusion; in the other 3 cases, TDF compliance was null at the time of infection (as demonstrated by TDF levels in blood).
Finally, in terms of efficacy data in real life, recently we have become aware of the confirmation of a significant reduction in new HIV infections among MSM, demonstrated since 2015 in 5 London clinics. This reduction would be justified by the use of PrEP, and at the same time by the effort made towards early diagnosis and treatment of new infections17,18.
All these data come to confirm those previously provided by clinical trials. After PrEP prescription, the incidence of HIV infection is low among a population where, given the high incidence of STI, it would be expected to find also a high incidence of new HIV infections. Likewise, these confirm the importance of treatment compliance, because PrEP is only effective when there is high adherence to treatment.
SafetyBoth TDF alone and in combination with FTC are well-tolerated drugs, seldom associated with the development of adverse effects at short and medium term. This rule seems to apply also in the case of PrEP, and its tolerability and safety can be considered satisfactory. In the majority of the studies reviewed, there were no clinically significant differences between the TDF or FTC/TDF arms and the placebo arms regarding the development of any adverse effects, grade 3 / 4 adverse effects, gastrointestinal disorders, diarrhoea, or discontinuation of the study due to adverse effects.5,9.
Particular attention must be paid to the potential development of renal toxicity associated with the use of TDF. A sub-analysis of the PARTNERS study analyzed specifically this potential toxicity19. After 18 months of follow-up, there was a change in the estimated glomerular filtration rate from -0.22, +0.14 or +1.37 mL/min/1.73 m2 in the FTC/TDF, TDF or placebo arms, respectively, and there was a >25% reduction in the estimated glomerular filtration rate over 18 months vs. the basal level in 0.41%, 0.25% or 0.83% of the FTC/TDF, TDF or placebo arms, respectively.
The use of TDF has also been associated with a loss in bone mineral density in those persons with HIV infection. A TDF2 sub-study assessed this potential loss in 109 persons who received FTC/TDF and 112 in the placebo arm. All of them underwent a basal densitometry, and then subsequent tests every 6 months20. Those persons who received FTC/TDF presented statistically significant worsening in T-scores or Z-scores throughout the study, both in lumbar spine as in hips. However, there were no differences in the incidence of bone fractures between both groups.
Regardless of this good profile of safety and tolerability, we must underline that those persons included in PrEP studies are young individuals, with few comorbidities, mostly male, and who received treatment during relatively short periods of time. However, according to data about the use of TDF during antiretroviral treatment, we know that TDF toxicity occurs at long term, typically after 3 to 5 years of treatment, and in persons with additional comorbidities such as hypertension or diabetes for renal toxicity, and women during menopause for the loss of bone mineral density. For these reasons, safety data for this strategy should be measured at long term, and with a longer follow-up.
Controversies: Prep failure, potential development of resistance mutations, and increase in STI diagnosisSince the start of antiretroviral therapy, we know that treatment with suboptimal therapies (monotherapy or dual) is associated with a high rate of development of resistance mutations. Their potential development during PrEP has been considered one of the major drawbacks that could appear. However, those studies conducted so far have not demonstrated an increase in resistance development with the use of PrEP. In a review that analyzed 10,045 persons included in different studies, 305 persons were infected during prophylaxis, and 18 of them (0.18% of the total number of persons included) presented resistance mutations21. However, half of those who developed some resistance mutation had been included in the study during their primary infection. Taking into account these facts, and excluding this group, there was a 0.9% resistance development among the total subjects included.
A case has been recently reported about a person infected with HIV while he was on PrEP, with good treatment compliance demonstrated through drug levels22. In this case, a resistance analysis demonstrated the presence of mutations to integrase inhibitor drugs (not included in the PrEP), while no mutations causing resistance to TDF were found: TDF is a drug included in the PrEP, and with high levels demonstrated in blood. Therefore, the conclusion of this case has been that this is not a failure in PrEP: this subject was exposed to a virus that already had resistance mutations, and this could not be prevented despite an adequate compliance with PrEP.
We know that viral replication is very high during the primary infection, and in these circumstances, monotherapy or dual therapy must be considered sub-optimal, and associated with a high development of resistance mutations. It has been calculated that there is a >25% development of resistance mutations in persons who were included in PrEP programs when they were already infected; this rate appears in contrast with the 0.09% previously stated23. As expected, the most frequently induced mutations were M184V/I and K65R, both in the reverse transcriptase gene. For this reason, follow-up must be conducted for those persons initiating PrEP, given the potential risk of developing resistance mutations in the early stage of an eventual seroconversion24,25.
Finally, given that no clinical trial or real-life study has demonstrated a 100% efficacy in PrEP, we must briefly discuss the likelihood of HIV transmission even if prophylaxis has been adequately prescribed and administered. This fact is so unusual that the confirmation of one HIV infection in the context of an adequate PrEP in one single person has deserved a recent communication to the scientific community26. This case has been observed in Amsterdam: a MSM male with a mean of 16 sexual contacts per month, consisting in anal sex without using condoms; there was a mean of 3.7 sexual partners in each contact. This repeated exposure to high-risk relationships without protection is the most likely cause for HIV infection regardless of an adequate PrEP.
Another potential controversy in the context of PrEP implementation is the fact that it might entail an increase in the transmission of other STIs. In a recent meta-analysis conducted in the University of California (UCLA), based on 18 cohort studies comparing a MSM population receiving PrEP vs. MSM who were not receiving PrEP, it was shown how the MSM arm on PrEP presented a risk 45 times higher of being diagnosed with 3 common STIs (syphilis, chlamydia and gonorrhoea) vs. the MSM arm not receiving PrEP27.
The potential risks, such as an increase in STI diagnosis in parallel with PrEP implementation, the potential infection by strains which already have resistance mutations, or potential infections by repeated exposure regardless of PrEP with adequate compliance, reinforce the need to continue conducting periodical screenings for STI, HIV and hepatitis, following the CDC recommendations.
ConclusionsPrEP is an effective and safe strategy for the prevention of HIV infection in persons at risk of said infection. Treatment compliance is particularly important in order to ensure its efficacy. However, there are still different issues that must be solved, such as improving its efficacy in women, long-term safety, or how to avoid its use during primary infection, in order to prevent an accumulation of resistance mutations.
IntroducciónSegún los últimos datos presentados referentes al número de nuevas infecciones por VIH en mayores de 13 años, en el periodo 2008-2014 la incidencia global ha disminuido en los Estados Unidos. Sin embargo, al analizar las diferentes poblaciones en riesgo de adquisición, se ha objetivado un incremento de nuevas infecciones en el grupo de hombres que tienen sexo con hombres (HSH) de edades comprendidas entre 25 a 34 años así como en mayores de 551.
En España, según datos del Ministerio de Sanidad, durante 2014 se comunicaron 3.366 nuevos casos de infección por VIH. Tras realizar la estimación, teniendo en cuenta el retraso existente en la notificación de los casos, se calcula que en 2014 se produjeron 9,34 nuevas infecciones por cada 100.000 habitantes siendo el 54% de ellos en HSH. Esto supone un incremento respecto a años anteriores en el grupo de población HSH de edades comprendidas entre los 20 a 30 años2.
Este incremento de nuevas infecciones en el grupo de HSH en un contexto de estabilidad global e incluso disminución en los nuevos casos durante los últimos años, es indicativo de la ausencia de eficacia de las medidas y campañas de prevención establecidas hasta el momento en dicho grupo. Es necesario por tanto implementar medidas preventivas alternativas, siendo la profilaxis farmacológica pre-exposición (PrEP) una de las opciones mejor evaluadas. A tener en cuenta, los resultados de los ensayos clínicos se han replicado de forma consistente en alguno de los lugares en los que se ha generalizado su uso en los casos indicados.
La administración de fármacos para prevenir una infección o sus consecuencias clínicas es una estrategia ya bien conocida y aplicada en medicina en situaciones diversas como la prevención de malaria administrando fármacos antipalúdicos o la administración de antibióticos como profilaxis quirúrgica. De forma similar, la base teórica de la PrEP se basa en la administración de antirretrovirales antes de que se produzca un contacto sexual que pudiera transmitir la infección por el VIH.
En este artículo haremos un breve repaso sobre los principales aspectos de esta estrategia, centrándonos fundamentalmente en la eficacia y seguridad de la misma.
Estudios sobre la eficacia de la PrEP como estrategia de prevención de la infección por VIHEl primer estudio que demostró la eficacia de la PrEP oral como estrategia de prevención frente al VIH fue el estudio iPrex publicado en el año 20103emtricitabine and tenofovir disoproxil fumarate (FTC-TDF. En este estudio se incluyeron 2.499 varones HSH seronegativos o mujeres transgénero (MTG) que tenían relaciones sexuales con hombres. Todos ellos fueron aleatorizados a recibir una combinación de emtricitabina y tenofovir disoproxil difumarato (FTC/TDF) o placebo una vez al día. Tras un año de seguimiento se habían infectado por VIH 36 personas en el grupo FTC/ TDF frente a 64 en el grupo placebo siendo la tasa de reducción de las nuevas infecciones de un 44% (IC95% 15-63) en el grupo de PrEP respecto al placebo.
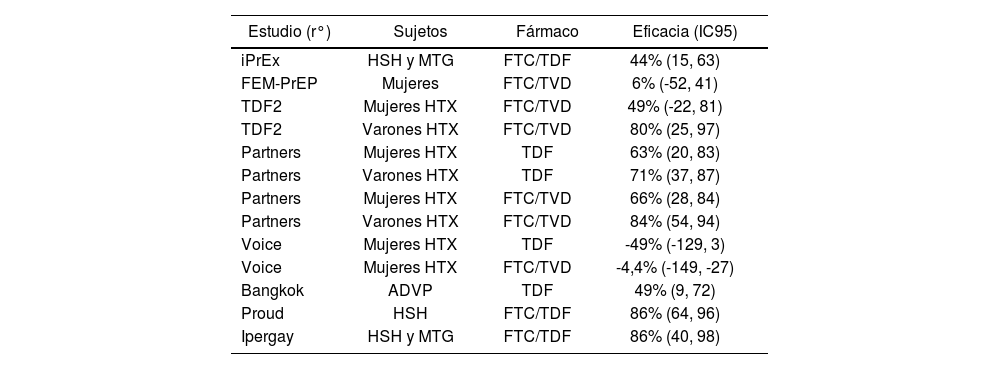
Tras este primer estudio se han ido realizando otros que han ido aportando más y mejores datos sobre la eficacia de esta estrategia de prevención. A continuación comentamos lo más relevante de ellos, estos datos se encuentran además resumidos en la tabla 1.
Principales ensayos clínicos publicados sobre PrEP
| Estudio (r°) | Sujetos | Fármaco | Eficacia (IC95) |
|---|---|---|---|
| iPrEx | HSH y MTG | FTC/TDF | 44% (15, 63) |
| FEM-PrEP | Mujeres | FTC/TVD | 6% (-52, 41) |
| TDF2 | Mujeres HTX | FTC/TVD | 49% (-22, 81) |
| TDF2 | Varones HTX | FTC/TVD | 80% (25, 97) |
| Partners | Mujeres HTX | TDF | 63% (20, 83) |
| Partners | Varones HTX | TDF | 71% (37, 87) |
| Partners | Mujeres HTX | FTC/TVD | 66% (28, 84) |
| Partners | Varones HTX | FTC/TVD | 84% (54, 94) |
| Voice | Mujeres HTX | TDF | -49% (-129, 3) |
| Voice | Mujeres HTX | FTC/TVD | -4,4% (-149, -27) |
| Bangkok | ADVP | TDF | 49% (9, 72) |
| Proud | HSH | FTC/TDF | 86% (64, 96) |
| Ipergay | HSH y MTG | FTC/TDF | 86% (40, 98) |
Otro de los estudios destacables, el estudio TDF2, patrocinado por los Centros de Control de Enfermedades de Atlanta (CDC), analizaba la utilización de FTC/TDF o placebo en mujeres y hombres seronegativos en Botswana y con relaciones sexuales de riesgo(4). Durante el seguimiento se produjeron 9 infecciones en el grupo de tratamiento (1,2 infecciones/100 personas año de seguimiento (pas) frente a 24 en el grupo placebo (3,1 infecciones/100 pas; lo que arroja una eficacia de la PrEP del 62,2% en este estudio (IC95%: 21,5-83,4).
El estudio Partners realizado en Kenia y Uganda incluyó 4.757 parejas heterosexuales serodiscordantes que fueron aleatorizadas a recibir TDF sólo, FTC/TDF combinado o placebo(5). Durante los 23 meses de seguimiento se produjeron 82 infecciones por VIH; 17 en el grupo TDF (0,65 episodios/100 personas año de seguimiento), 13 en el grupo FTC/ TDF (0,50/100 personas año de seguimiento) y 52 en el grupo placebo (1,99/100 personas año de seguimiento). Por lo tanto el uso de TDF tuvo una protección del 67% respecto al grupo placebo (IC95% 44-81) y la protección fue del 75% (IC95% 55-87) para el grupo FTC/TDF.
A partir del año 2015 se comunicaron datos también de estudios realizados en Europa. Los dos más importantes fueron en primer lugar el estudio PROUD6. En él se incluyeron 544 HSH aleatorizados a recibir 1 comprimido diario de FTC/TDF de manera inmediata o a diferir su inicio 12 meses. Todos los participantes fueron instruidos con consejos para reducir el riesgo durante las relaciones sexuales y se suministraron preservativos durante todo el estudio. A lo largo del seguimiento, ambos grupos presentaron una alta incidencia de ITS y sin diferencias estadísticas entre ellos. El estudio fue suspendido por el comité de seguridad al comprobar que las personas en las que se difería el inicio de la profilaxis tenían un mayor riesgo de infección por VIH que las que lo hacían de manera inmediata. En el grupo de tratamiento inmediato se produjeron 3 infecciones, frente a 20 en el grupo diferido (9,0/100 personas-año) y con una reducción del 86% (IC90% 6496). Según estos datos sería necesario dar la profilaxis a 13 personas para evitar una nueva infección por VIH. De las tres personas que se infectaron en el brazo de tratamiento inmediato, una entró en el estudio ya infectada (serología negativa pero PCR-VIH positiva en el basal); mientras que las otras dos habían dejado de tomar la profilaxis tiempo antes de la infección.
El segundo trabajo es el estudio Ipergay, realizado en Francia y Canadá, y en el que se incluyeron 400 varones HSH o mujeres transgénero (MTG) no infectados por VIH y con alto riesgo de infección7. Tras la inclusión fueron aleatorizados a recibir profilaxis con FTC/TDF o con placebo. En este caso la profilaxis se realizaba a demanda con la administración de 2 comprimidos de FTC/TDF entre 2-24 horas antes de mantener una relación sexual, seguido de 1 comprimido a las 24 horas y otro a las 48 horas de dicha relación. En el caso que se siguieran teniendo relaciones sexuales se continuaba con 1 comprimido diario hasta las 48 horas de la última relación. Si con posterioridad se volvían a mantener relaciones sexuales, se iniciaba de nuevo la profilaxis con 2 comprimidos de FTC/TDF seguidos de 1 comprimido diario hasta 48 horas después de la última relación. El brazo control recibió el mismo esquema, aunque con un placebo. Al igual que en el estudio PROUD todos los participantes fueron instruidos para minimizar el riesgo durante las relaciones sexuales y se facilitaron preservativos durante todo el seguimiento. De nuevo la incidencia de ITS durante el seguimiento fue elevada lo que habla a favor del mantenimiento de relaciones de alto riesgo en ambos brazos del estudio. Al igual que en el estudio PROUD, el comité de seguridad suspendió el estudio a los 9 meses de su inicio, ya que durante el seguimiento se produjeron 2 infecciones por VIH en el grupo de estudio (0,91 infecciones/100 personas-año) frente a 14 en el grupo placebo (6,6/100 personas-año). La efectividad de la profilaxis fue del 86% (IC95% 40-98, p=0,002), siendo necesario tratar a 18 personas para prevenir 1 nueva infección. De nuevo ninguna de las dos personas infectadas en el grupo FTC/TDF tenía niveles detectables de TDF en sangre.
El estudio HPTN 067 / ADAPT (Alternative Dosing to Augment PrEP Pill-Taking) es un ensayo clínico en fase II diseñado para comprobar si las pautas intermitentes de PrEP podrían facilitar su cumplimentación8 US. El estudio se llevó a cabo en 3 poblaciones diferentes: HSH de Bangkok, HSH de Harlem y mujeres heterosexuales de Ciudad del Cabo. En las tres ramas los participantes fueron aleatorizados a recibir 1 comprimido diario de TDF/FTC o 1 comprimido intermitente en función del tiempo (1 comprimido 2 veces por semana más 1 comprimido extra tras cada contacto sexual) o en función de la actividad sexual (1 comprimido antes y 1 comprimido después de cada contacto sexual). En los tres subgrupos la profilaxis diaria consiguió mejores tasas en la reducción de nuevas infecciones demostrando además una mejor adherencia. De forma global la cohorte de Harlem fue la que peor respuesta alcanzó (65% cohorte Harlem, 85% cohorte Bangkok, 75% cohorte Ciudad del Cabo).
Frente a estos trabajos que sí han demostrado eficacia de la PrEP, se han comunicado otros en los que esta eficacia ha sido cuestionada. El estudio FEM-Prep incluyó 2.120 mujeres seronegativas en Kenia, Sudáfri- ca y Tanzania que fueron aleatorizadas a FTC/TDF o placebo9. En total, 33 mujeres se infectaron en el grupo FTC/TDF (incidencia 4,7 infeccio- nes/100 personas año seguimiento [pas]) frente a 35 en el grupo placebo (5 infecciones/100 pas) con un HR de protección del 0,94 (IC95% 0,59 - 1,52). En el estudio Voice, realizado en Sudáfrica, Zimbabue y Uganda se incluyeron 5.029 mujeres seronegativas que se aleatorizaron a TDF sólo, FTC/TDF, gel vaginal de TDF al 1% y dos grupos placebo uno de tratamiento oral y otro del gel vaginal10. En total se produjeron 312 infecciones con una incidencia de 5,7/100 pas. En esta ocasión, ninguno de los 3 brazos de estudio, resultaron protectores frente al placebo. La efectividad del TDF administrado como único fármaco solo fue de -49%, la de FTC/TDF fue de -4,4% y finalmente la del gel vaginal 14,5%, aunque en este último caso sin significación estadística.
Fuera de la transmisión sexual, un estudio realizado en Bangkok mostró un nivel de protección del 48,9% (IC95% 9,6-72,2), entre 2.413 personas adictas a drogas por vía parenteral y no infectados por VIH que fueron aleatorizados a recibir TDF o al grupo control11.
En la mayoría de casos, las diferencias en la eficacia de la PrEP entre los diferentes estudios, estriban en las diferencias de cumplimientos terapéuticos. Por ejemplo, en el estudio Voice, que no demostró la eficacia de la PrEP, los niveles de TDF fueron detectados únicamente en el 30%, 29% y 25% de las pacientes aleatorizadas a recibir TDF, FTC/TDF o gel de TDF10. De igual manera, solo el 28% de las mujeres asignadas a FTC/TDF tenían niveles detectables de FTC en el estudio FEM-PrEP9. En un subanálisis del estudio iPrex cuando se comparaba aquellas personas aleatorizadas a recibir FTC/TDF que se infectaban por VIH con los que no se infectaban, aquellos tenían menores niveles de TDF, tanto en la visita de la serocon- versión (8% vs 44%, p<0,001), como en la de los 90 días previos (11% vs 51%, p<0,001)9. De hecho, en los que presentaban concentraciones de TDF detectables en células de sangre periférica se demostró una reducción del 90% en el riesgo de adquisición de VIH.
Datos parecidos se encontraron en el estudio PARTNERS, en este caso entre las personas infectadas solo el 21% tenían niveles considerados como protectores (>40 ng/mL) frente al 71% de los no infectados5. Incluso, en aquellas personas que superaban dicha concentración la efectividad de la profilaxis fue del 88% (IC95% 60-96) para las que recibían TDF y 91% (IC95% 47-98) para las que recibían FTC/TDF.
Por último, en el estudio realizado en Bangkok entre ADVP, cuando el análisis se restringía a personas con buen cumplimiento terapéutico y que tuvieran niveles detectables de TDF, la eficacia subió hasta el 73,5% (IC95% 16,6-94)11
Además de la baja adherencia como causa clara del fallo de la PrEP, algunos trabajos podrían indicar que hay también diferencias farmacológicas que explicaran estas discrepancias. Por ejemplo, tras la administración de PrEP se ha comprobado que los niveles de TDF en tejido rectal de varones son entre 10-100 veces mayores que los alcanzados en tejido cer- vicovaginal de mujeres, lo cual podría hablar a favor de una peor eficacia de la PrEP entre las mujeres12.
Datos de PrEP en la vida realTras los primeros ensayos clínicos publicados, la FDA aprobó en 2012 la utilización de la PrEP y en 2014 los CDC realizaron unas recomendaciones de su utilización13. En la actualidad se han comunicado diversos estudios sobre su uso en la vida real y no parece que en estas circunstancias los resultados se alejen mucho de lo comunicado en los ensayos clínicos. En datos comunicados del área de San Francisco dentro de la aseguradora Kaiser Permanente en el periodo entre julio de 2012 y febrero de 2015, tras la prescripción de PrEP a 657 personas con un seguimiento de 388 perso- nas/año, y a pesar de presentar un alto porcentaje de diagnósticos de ITS (28% de las personas presentaron al menos una ITS durante el seguimiento), no hubo ningún caso de infección por VIH14.
En el estudio DEMO Project realizado en clínicas de San Francisco y Miami se administró PrEP a 557 HSH y MTG entre octubre de 2012 y enero de 201415.Se produjeron un total de 5 infecciones por VIH; tres de las cuales fueron consideradas como primoinfecciones presentes en el momento de la inclusión y solo hubo 2 a lo largo del seguimiento (incidencia de 0,43/100 pas). Una vez más, ninguno de estos dos últimos participantes tenía niveles protectores de TDF en sangre en el momento de la infección.
Merece la pena resaltar el estudio ATN 110 que analiza la utilización de PrEP en una población de 200 HSH entre 18-22 años16. En total se produjeron 4 episodios de infección VIH (3,29/100 pas). En uno de ellos se demostró que el paciente había iniciado su participación en el estudio ya infectado por VIH, en los otros 3 casos la adherencia al TDF fue nula en el momento en el que se produjo la infección (demostrada por niveles de TDF en sangre).
Por último, respecto a datos de eficacia en vida real hemos conocido muy recientemente la confirmación del descenso significativo de nuevas infecciones por VIH en HSH demostrada desde el año 2015 en 5 clínicas de Londres. Este descenso estaría justificado por una combinación de estrategias consistente en incrementar la utilización de la PrEP de forma paralela a la realización de un esfuerzo en el diagnóstico y tratamiento precoz de las nuevas infecciones17,18.
Todos estos datos vienen a confirmar los aportados previamente por los ensayos clínicos. Tras la prescripción de PrEP, la incidencia de infección VIH es baja en un colectivo en el que, a la vista de la alta incidencia de ITS, cabría esperar también una alta incidencia de nuevas infecciones por VIH. De igual manera confirman la importancia que tiene el cumplimiento terapéutico ya que la PrEP es efectiva únicamente si hay una alta adherencia al tratamiento.
SeguridadTanto TDF solo como en combinación con FTC son fármacos bien tolerados y poco asociados con el desarrollo de efectos adversos en el corto y medio plazo. Esta norma parece seguir cumpliéndose en el caso de la PrEP y tanto la tolerancia como la seguridad de los mismos puede considerarse como satisfactoria. En la mayoría de los estudios analizados no existieron diferencias clínicamente significativas entre los grupos TDF o FTC/TDF y los grupos placebo respecto a aparición de cualquier efecto adverso, efectos adversos grado 3/4, trastornos gastrointestinales, diarrea o discontinuación del estudio por efectos adversos5,9.
Especial atención merece la posible aparición de toxicidad renal asociada con el uso de TDF. Un subanálisis del estudio PARTNERS analizó específicamente esta posible toxicidad19. Tras 18 meses de seguimiento se produjo un cambio del filtrado glomerular estimado de -0,22, +0,14 o +1,37 mL/min/1,73 m2 en los grupos FTC/TDF, TDF o placebo respectivamente y se produjo una disminución >25% del filtrado glomerular estimado a lo largo de los 18 meses respecto al basal en el 0,41%, 0,25% o 0,83% de los grupos FTC/TDF, TDF o placebo respectivamente.
El uso de TDF, también se ha sido asociado con una pérdida de la densidad mineral ósea en personas infectadas por VIH. Un subestudio del TDF2 valoró esta posible pérdida en 109 personas que recibieron FTC/ TDF y 112 del grupo placebo. A todos ellos se les realizó una densitometria basal y cada 6 meses con posterioridad20. Las personas que recibieron FTC/TDF presentaron un empeoramiento estadísticamente significativos de los T-scores o Z-scores a lo largo del estudio tanto en la columna lumbar como en la cadera. Sin embargo, no hubo diferencias en la incidencia de fracturas óseas entre ambos grupos.
A pesar de este buen perfil de seguridad y tolerancia hay que reseñar que las personas incluidas en los estudios de PrEP son individuos jóvenes, con pocas comorbilidades, mayoritariamente varones y que reciben el tratamiento durante periodos relativamente cortos de tiempo. Sin embargo, de los datos conocidos del uso de TDF durante el tratamiento antirretroviral sabemos que la toxicidad de TDF se produce en el largo plazo, normalmente por encima de 3-5 años de tratamiento, y en personas que tienen comorbilidades añadidas como hipertensión o diabetes para la toxicidad renal y mujeres durante la menopausia para la pérdida de la densidad mineral ósea. Por estas razones, los datos de seguridad de esta estrategia debería ser medida en el largo plazo y con un seguimiento más prolongado de los mismos.
Controversias: Fracaso de la prep, posibilidad de aparición de mutaciones de resistencia e incremento en el diagnóstico de ITSDesde los inicios del tratamiento antirretroviral sabemos que el tratamiento con terapias subóptimas (mono o biterapias) se asocian con un alto índice de desarrollo de mutaciones de resistencia. Su posible aparición durante la PrEP, se ha considerado como uno de los inconvenientes mayores que se podrían presentar. Sin embargo, de los estudios realizados hasta el momento no se ha demostrado un incremento en la aparición de resistencias en la utilización de la PrEP. En una revisión y analizando 10.045 personas incluidas en varios estudios, 305 personas se infectaron durante la profilaxis y de ellas, 18 (0,18% del total de incluidos) presentaron mutaciones de resistencia (21). Sin embargo, la mitad de los que desarrollaron alguna mutación de resistencia eran sujetos que habían sido incluidos en el estudio durante su primoinfección. Teniendo en cuenta estos hechos, y excluyendo a este grupo, el desarrollo de resistencias fue de 0,09% del total de sujetos incluidos.
Recientemente se ha comunicado un caso de un individuo infectado por VIH mientras estaba tomando PrEP con buena adherencia demostrada mediante niveles de fármacos22. En este caso, tras realizar el análisis de resistencias se demostró la presencia de mutaciones a fármacos inhibidores de la integrasa (no incluidos en la PrEP) mientras no se encontraron mutaciones que confirieran resistencia al TDF, fármaco incluido en la PrEP y con niveles elevados demostrados en sangre. La conclusión por tanto de este caso ha sido que no se trata de un fallo en la PrEP, el individuo se expuso a un virus ya con mutaciones de resistencia que no pudieron ser evitadas a pesar del cumplimiento correcto de la PrEP.
Durante la primoinfección sabemos que la replicación vírica es muy alta y en estas circunstancias la mono o biterapia debe considerarse como subóptima y asociada con un alto desarrollo de mutaciones de resistencias. Se ha calculado que la aparición de mutaciones de resistencia en personas que entraron ya infectadas en los programas de PrEP es superior al 25%, cifra que contrasta con el 0,09% antes expuesto23. Como era de esperar las mutaciones más frecuentemente inducidas fueron la M184V/I y la K65R ambas en el gen de la transcriptasa inversa. Por esta razón, se debe realizar un seguimiento de los individuos que inician PrEP dado el posible riesgo de desarrollar mutaciones de resistencia en la fase precoz de una eventual seroconversión24,25.
Finalmente, dado que en ningún ensayo clínico ni estudio de vida real se ha demostrado una eficacia de la PrEP del 100%, no podemos dejar de comentar brevemente la posibilidad de que haya transmisión del VIH aunque la profilaxis se esté prescribiendo y tomando correctamente. Este hecho es tan inusual que la constatación de una infección por VIH en el contexto de PrEP adecuada en un único individuo ha merecido una comunicación reciente a la comunidad científica26. El caso al que hacemos referencia se ha objetivado en Amsterdam y se trata de un varón HSH con una media de 16 encuentros sexuales al mes practicando sexo anal sin utilización de preservativo siendo la media de parejas sexuales en cada uno de los encuentros de 3,7. Esta exposición reiterada a relaciones de alto riesgo sin protección es la causa más probable de que se produjera la infección por VIH a pesar de una adecuada PrEP.
Otra de las posibles controversias que surgen en el seno de la implantación de la PrEP es el hecho de que dicha implantación puede conllevar un incremento en la transmisión de otras ITS. En un reciente metanálisis llevado a cabo en la Universidad de California (UCLA) a partir de 18 estudios de cohortes comparando población HSH recibiendo PrEP frente a HSH que no recibe PrEP, se muestra como el grupo de HSH en PrEP presenta un riesgo 45 veces superior de ser diagnosticado de tres ITS comunes (sífilis, chlamydia y gonorrea) respecto al grupo de HSH que no recibe PrEP(27).
Los posibles riesgos como son, el incremento del diagnóstico de ITS de forma paralela a la implementación de PrEP, posibilidad de contagio por cepas ya con mutaciones de resistencia, o posibles contagios por exposición reiterada a pesar de PrEP con adecuado cumplimiento, reafirman la necesidad de no dejar de hacer cribados periódicos de ITS, VIH y hepatitis tal y como está recomendado por los CDC.
ConclusionesLa PrEP es una estrategia eficaz y segura en la prevención de la infección por VIH en personas en riesgo de adquirir dicha infección. El cumplimiento terapéutico es de especial importancia para asegurar la eficacia de la misma. Sin embargo, quedan todavía por resolver diferentes cuestiones como mejorar su eficacia entre las mujeres, la seguridad a largo plazo o como evitar su utilización durante la primoinfección para evitar el acúmulo de mutaciones de resistencias.


Farmacia Hospitalaria sigue las recomendaciones para la preparación, presentación y publicación de trabajos académicos en revistas biomédicas
- Inicio
- Todos los contenidos
- Publique su artículo
- Acerca de la revista
- Métricas