

To define recommendations that permit safe management of antineoplastic medication, minimise medication errors and improve the safety of cancer patients undergoing treatment.
MethodBy reviewing the literature and consulting the websites of various health organisations and agencies, an expert committee from the Spanish Society of Hospital Pharmacy and the Spanish Society of Medical Oncology defined a set of safe practices covering all stages of providing cancer therapy to patients. The Spanish Society of Oncology Nursing revised and endorsed the final list.
ResultsIn total, 68 recommendations arranged in 5 sections were defined. They include issues concerning the training of health professionals, the technological resources needed, treatment planning, informing the patient and his family, the processes of prescribing, preparing, dispensing and administering cancer therapy (orally, parenterally or intrathecally), assessing patient adherence and treatment toxicity.
ConclusionsIt is essential for healthcare establishments to implement specific measures designed to prevent medication errors, in order to ensure the safety of cancer patients treated with antineoplastic medication.
Definir unas recomendaciones que permitan el manejo seguro de la medicación antineoplásica, minimizar los errores de medicación y mejorar la seguridad de los pacientes oncológicos tratados.
MétodoA partir de una revisión de la bibliografía, así como de la consulta de páginas web de varias agencias y organismos sanitarios, un comité de expertos de la Sociedad Española de Farmacia Hospitalaria y la Sociedad Española de Oncología Médica han definido una serie de prácticas seguras para todas las etapas de la provisión del tratamiento antineoplásico al paciente. La Sociedad Española de Enfermería Oncológica revisó y respaldó la lista final.
ResultadosSe han definido 68 recomendaciones estructuradas en 5 secciones. Se incluyen aspectos relacionados con la formación de los profesionales sanitarios; los recursos tecnológicos necesarios; la planificación del tratamiento; la información al paciente y a sus familiares; los procesos de prescripción, preparación, dispensación y administración del tratamiento antineoplásico (por vía oral, parenteral o intratecal), así como la evaluación de la adherencia del paciente y la toxicidad del tratamiento.
ConclusionesEl establecimiento de medidas concretas destinadas a prevenir los errores de medicación en los centros sanitarios es esencial para garantizar la seguridad de los pacientes oncológicos tratados con medicación antineoplásica.
The rising incidence and prevalence of cancer, and the rapid development of new treatment strategies, have resulted in greater diversity and complexity of cancer therapies in recent years. Because of improved survival and quality-of-life outcomes in many cancers, together with greater use of the oral route and better tolerability of many new drugs, increasing numbers of patients are receiving cancer therapy in oncology departments. This situation poses new challenges for achieving safe management of cancer drugs by the health professionals involved.
For decades, cancer therapy (particularly chemotherapy) has been the prime example of high-risk medication. The risk of fatality or serious complications entailed in chemotherapy1, including cases with major social repercussions such as intrathecal delivery errors2, has led the scientific community to introduce hitherto unheard-of multidisciplinary practices for validating and double-checking treatment, in order to improve cancer patient safety34. With the aim of preventing various types of errors and risks of adverse effects in patients, a wide range of recommendations have been published in recent years56. They include standardisation of treatment orders7, safe labelling8–10, checklists11 or, more recently, computer order entry systems integrated with electronic health records and machine-readable coding during administration12–15. All these measures have contributed greatly to improving safety16, but do not entirely guarantee it17. Those recommendations were subsequently incorporated into national and international standards and guidelines5,18–23 by the American Society of Clinical Oncology (ASCO) and the Oncology Nursing Society (ONS)24–26, the American Society of Health-System Pharmacists (ASHP)27 and the Institute for Safe Medication Practices (ISMP), among others2829. Complying with certain standards is a mandatory requirement in current cancer care quality systems30.
However, in the context of growing patient safety demands and rapid introduction of new treatments, establishing safe basic procedures may not be enough. In particular, the advent of oral drugs for non-hospital use has not been accompanied by the same safety requirements now in place for intravenous chemotherapy in the oncology hospital setting31. That has generated new risks and challenges in cancer patient care, such as monitoring adherence and educating patients about their treatment3233, resulting in new recommendations specifically for oral therapy3435, now included in the latest versions of international publications242527.
In Spain, no consensus document is yet available in which a full set of multidisciplinary measures is defined for the safe treatment of cancer patients with antineoplastic drugs. Some advisable practices are contained in other reports, such as the recent Strategic Plan for Pharmaceutical Care in Oncology/Haematology Patients by the Spanish Group for the Development of Oncology Pharmacy (GEDEFO)36 or the document on oncology day hospitals produced by the Spanish Society of Medical Oncology (SEOM)3738.
The aim of this work has been to define a set of multidisciplinary safety recommendations for managing antineoplastic medications, to help prevent medication errors and improve the safety of cancer patients in Spain.
MethodsThese consensus recommendations are based on a review of the available evidence about safe practices in cancer therapy, and the professional opinions of the Spanish Society of Medical Oncology (SEOM), the Spanish Society of Hospital Pharmacy (SEFH) and Spanish Society of Oncology Nursing (SEEO) experts.
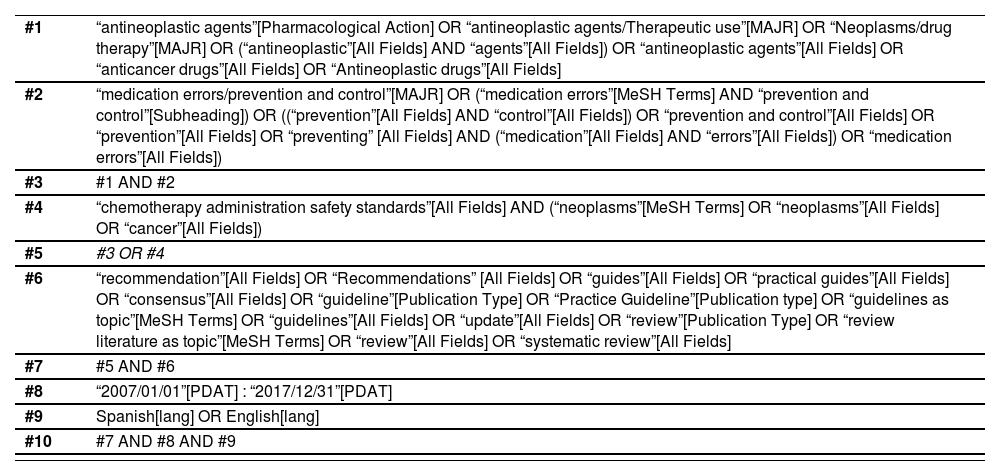
Literature reviewIn order to identify safe practices regarding antineoplastic drug management, a structured literature search was performed in the PubMed database for publications on cancer therapy recommendations and safety and quality standards. The search was confined to articles published in English or Spanish between 1 January 2007 and 31 May 2017. The search syntax employed included the combination of MeSH descriptors and key words or text words shown in Table 1. This search identified 85 publications, from which 23 in total were finally selected by reading the abstracts1,2,4,6,7,9,11–13,16–19,24,25,27,28,30–33,35,39.
Search strategy in PubMed
| #1 | “antineoplastic agents”[Pharmacological Action] OR “antineoplastic agents/Therapeutic use”[MAJR] OR “Neoplasms/drug therapy”[MAJR] OR (“antineoplastic”[All Fields] AND “agents”[All Fields]) OR “antineoplastic agents”[All Fields] OR “anticancer drugs”[All Fields] OR “Antineoplastic drugs”[All Fields] |
| #2 | “medication errors/prevention and control”[MAJR] OR (“medication errors”[MeSH Terms] AND “prevention and control”[Subheading]) OR ((“prevention”[All Fields] AND “control”[All Fields]) OR “prevention and control”[All Fields] OR “prevention”[All Fields] OR “preventing” [All Fields] AND (“medication”[All Fields] AND “errors”[All Fields]) OR “medication errors”[All Fields]) |
| #3 | #1 AND #2 |
| #4 | “chemotherapy administration safety standards”[All Fields] AND (“neoplasms”[MeSH Terms] OR “neoplasms”[All Fields] OR “cancer”[All Fields]) |
| #5 | #3 OR #4 |
| #6 | “recommendation”[All Fields] OR “Recommendations” [All Fields] OR “guides”[All Fields] OR “practical guides”[All Fields] OR “consensus”[All Fields] OR “guideline”[Publication Type] OR “Practice Guideline”[Publication type] OR “guidelines as topic”[MeSH Terms] OR “guidelines”[All Fields] OR “update”[All Fields] OR “review”[Publication Type] OR “review literature as topic”[MeSH Terms] OR “review”[All Fields] OR “systematic review”[All Fields] |
| #7 | #5 AND #6 |
| #8 | “2007/01/01”[PDAT] : “2017/12/31”[PDAT] |
| #9 | Spanish[lang] OR English[lang] |
| #10 | #7 AND #8 AND #9 |
The literature search was supplemented by a manual search for secondary references cited in the articles initially selected 3,5,8,15,34. A manual search for documents about standards or recommendations for safe practices with cytostatics was also performed on the websites of the following health organisations and agencies:
Initial selection of safe practices by an expert committeeFor the production of this document, SEOM and SEFH set up a committee of experts in cancer therapy and drug safety, composed of four specialists from each society.
The first stage involved the experts analysing the publications selected during the literature search, in order to identify and compile safe practices covering all stages of cancer therapy provision. The expected benefits were taken into account, as was the feasibility of incorporation into Spanish healthcare practice. This stage identified 74 safe practices, which were discussed and screened at a meeting attended in person by the expert committee members. Several rounds of revision then took place between the committee members, working remotely. At the end of this process, 68 practices were selected in total.
Revision of selected practices by independent professionals, and production of the consensus statement
The expert committee drafted a set of recommendations for the safe management of cancer medication, containing the 68 selected practices. This draft was e-mailed to various health professionals belonging to SEFH and SEOM, who had been chosen in advance for their knowledge of this field. They were asked for comments and suggestions about the practices included, in terms of content and wording. They were also given the opportunity to suggest the inclusion of new practices.
All the comments and suggested amendments to the contents and form of the document, sent by the health professionals consulted, were analysed and discussed by the expert committee until an agreed draft list of safe practices was achieved.
This draft list of safe practices was then submitted for review and endorsement to the SEEO, which suggested additional comments and amendments to clarify some practices. These amendments were discussed by the expert committee and were included in the final document.
ResultsTable 2 contains the full list of safe practices for the management of cancer therapy agreed by this expert committee. This list includes 68 practices divided into 5 sections, following a scheme like the one used in the ASCO/ONS chemotherapy administration safety standards24. Section 1 contains 17 general measures intended for healthcare establishments, about the training of health professionals involved in cancer patient treatment, the human and technological resources needed, the standard operating procedures that should exist, and procedures for continuity of care and risk management. Section 2 supplements the above with 9 practices related to cancer therapy planning, informed consent, and informing the patient and his family or carers about medication.
SEFH//SEEO/SEOM antineoplastic drugs safety recommendations
|
Section 3 contains 33 practices addressing the stages of prescribing, preparing, dispensing and administering oral and parenteral cancer therapy, including specific measures for intrathecally delivered medication. This section is supplemented by Section 4, which contains 5 practices on treatment monitoring, including the assessment of patient adherence and cancer treatment toxicity. Lastly, the 4 practices in Section 5 briefly highlight the importance of ensuring the safety of health professionals who prepare and administer antineoplastic medication. It was decided that in-depth consideration of this issue was beyond the scope of this document, because it did not form part of the initial aim of these recommendations.
DiscussionMedication safety management is a critical aspect of cancer patient care. Because antineoplastic drugs have a narrow therapeutic range, medication errors that can arise for various reasons during the course of treatment carry a high risk of causing patients serious adverse effects or compromising the clinical benefit of therapy. Safe practices to minimise them and prevent unnecessary harm to patients must therefore be implemented. Aware of this need, SEFH and SEOM have worked closely together to produce a multidisciplinary document that brings together a set of fundamental practices to ensure the safety of cancer patient care. Starting from a literature review, an expert committee produced a set of recommendations tailored to Spain. These were revised by a group of independent professionals from both societies and endorsed by the SEEO.
The recommendations are intended for healthcare establishments and professionals who provide parenteral and oral cancer therapy, either with commercially available medications or with clinical research products. The recommendations address all stages involved in the process of providing cancer drug treatment, from prescribing to patient monitoring. Additionally, they cover other measures considered essential for improving cancer patient safety, some of which entail profound change in an organisation's culture. Examples include continuing professional development and assessment of competence, standardisation of all working procedures and healthcare protocols, and setting up risk management systems. All of these are crucial for improving safety. These recommendations also incorporate the minimum technological and human resources that need to be available at healthcare centres in order to reduce variability of care provided, ensure fairness, and assure the safety of cancer therapy.
Today, cancer is regarded as a chronic disease, and oral antineoplastic therapies are increasingly used. Together, these two facts have required patient care strategies to change direction, towards a cooperative multidisciplinary model, in which it is particularly important to inform and talk to the patients and/or carers who will have to be actively involved in treatment. One whole section of recommendations is therefore devoted to this. The document contains other fundamental practices in these patients, such as monitoring adherence and reconciling treatments during transitions of care.
The practices listed in this consensus statement are not intended as safety standards for healthcare establishments, because the scientific societies that produced them do not provide certification. Nevertheless, these specific measures aimed at preventing medication errors should obviously be adapted and implemented by healthcare establishments, in order to improve the safety of the care they provide. This document is also intended to assist health professionals, who can use the recommendations as a benchmark for their healthcare practice.
Lastly, it should be noted that SEFH, SEOM and SEEO intend to promote the development of initiatives to encourage the introduction of these recommendations, and to update them periodically, when new practices are developed that affect the safety of cancer therapy. The aim is for patients receiving antineoplastic therapy in Spain to do so with maximum assurances of quality and safety.
FundingThis project was supported with unrestricted grants from SEFH and SEOM.
AcknowledgementsThe authors thank the following experts who reviewed and contributed with suggestions to the content of this manuscript: Carmen Beato, Monica Carbajales, Ignacio García-Escobar, José A Marcos, Javier Pérez-Altozano, Montserrat Pérez-Encinas, José A Pérez-Fidalgo, Cesar A Rodríguez, María Dolores Santos-Rubio and Inmaculada Torre-Lloveras.
The authors also wish to thank Helena Martín, Head of Bio-health Libraries at the University of Salamanca, for her contribution to the search strategy for the literature review. Editorial assistance for the development of this manuscript was provided by Beatriz Gil-Alberdi of HealthCo (Madrid, Spain).
Conflict of interestsNo conflict of interests.
Grupo de Traba¡o SEFH-SEEO-SEOM para la seguridad del paciente oncológico
María José Otero, Instituto para el Uso Seguro de los Medicamentos (ISMP-España), Servicio de Farmacia Hospitalaria, Hospital Universitario de Salamanca, Salamanca, España; Ruth Vera, Servicio de Oncología Médica, Complejo Hospitalario de Navarra, Pamplona, España; Cristina González-Pérez, Servicio de Farmacia Hospitalaria, Hospital Clínico San Carlos, Madrid, España; Francisco Ayala de la Peña, Servicio de Hematología y Oncología Médica, Hospital General Universitario Morales Meseguer, Murcia, España; Ángeles Peñuelas, Coordinadora de Enfermería Oncológica, Hospital Universitari Vall d'Hebron, Vall d'Hebron Instituto de Oncología, Barcelona, España; Nuria Quer, Servicio de Farmacia Hospitalaria, Instituto Catalán de Oncología, Barcelona, España; Juan Manuel Sepúlveda, Servicio de Oncología Médica, Hospital Universitario Doce de Octubre, Madrid, España; Nuria Doménech-Climent, Adjunta de Enfermería, Hospital Virgen de los Lirios, Alcoy, Profesora Asociada, Universidad de Alicante, Alicante, España; Juan Antonio Virizuela, Servicio de Oncología Médica, Hospital Universitario Virgen Macarena, Sevilla, España; Patricia Beorlegui, Enfermería Clínica Avanzada, Clínica Universitaria de Navarra, Pamplona. España; María Queralt Gorgas, Servicio de Farmacia Hospitalaria, Hospital Universitario Vall d'Hebron, Barcelona, España.

