














To describe the implementation of a pilot Telepharmacy project (TELEA-Farmacia) in adult patients with cancer, analyze the results obtained, and identify opportunities for improvement, from a hospital pharmacy service.
MethodBetween October and December 2021, oncology patients, collecting their oral antineoplastic drugs at the Unit of Oncology Pharmacy of the hospital pharmacy service were stratified using the MAPEX model. Oncology patients candidates for inclusion in the TELEA-Farmacia project included “medium-high priority” hospital pharmacy patients, along with oncology patients who, according to pharmacist's opinion, could benefit from Telepharmacy. On a weekly basis, oncology patients recorded on the TELEA platform their biological measurements and completed the questionnaires on medication adherence and pain. Questionnaires on quality of life were completed on a monthly basis. To score health indicators, oncology patients accessed TELEA through the SERGAS-MOBIL app or a web browser. Follow-up of health indicators was performed by the Unit of Oncology Pharmacy of the hospital pharmacy service.
ResultsThe study sample included 29 oncology patients (48% were male) with a mean age of 59 years (44-75). According to the stratification model, 31% were low-priority patients, 62% had medium-priority, and 7% had high priority. The digital gap in patients with advanced ages was the main obstacle to inclusion. Reports were monitored daily, and a total of 364 responses were received. In the presence of alarming reports and/or out-of-range values, active monitoring and/or telephonic follow-up were initiated. Pharmaceutical care was adapted to the health problem detected according to individual patient needs.
ConclusionsThe Telemedicine pilot project TELEA-Farmacia made it possible to test TELEA in patients with cancer in a real-life context. TELEA facilitated continuous follow-up, early detection of drug-related problems, and the identification of new needs and improvement points. To such purpose, clinical oncology pharmacists combined face-to-face consults with patient stratification and remote follow-up. This study demonstrated that new stratification models are necessary in hospital pharmacy services to identify patients with technology skills who can benefit from using Telemedicine tools as TELEA.
Describir la implantación de un proyecto piloto de Telefarmacia (TELEA-Farmacia) en el paciente oncológico adulto y analizar los resultados recabados, así como identificar las oportunidades de mejora, desde un servicio de farmacia hospitalario.
MétodoEntre octubre y diciembre de 2021, los pacientes oncológicos a tratamiento con antineoplásicos orales citados en la consulta de farmacia oncológica del servicio de farmacia de hospital fueron estratificados a través del modelo MAPEX. Se consideraron susceptibles de inclusión en TELEA-Farmacia a quienes requerían atención farmacéutica con “prioridad media-alta” y a aquellos que, según criterio farmacéutico, pudieran beneficiarse de la herramienta. A través del aplicativo TELEA se programaron semanalmente biomedidas y cuestionarios de adherencia y evaluación del dolor, y mensual-mente un cuestionario de calidad de vida. Accediendo a TELEA mediante la aplicación móvil SERGAS-MÓBIL o un navegador web, los pacientes oncológicos respondieron a los indicadores de salud programados, de cuyo seguimiento fue responsable la Unidad de Farmacia Oncológica del servicio de farmacia de hospital.
ResultadosSe incluyeron 29 pacientes oncológicos (48% hombres), con una media de 59 años (44-75). Un 31% fueron de prioridad baja, 62% media y 7% alta según el modelo de estratificación, siendo la brecha digital existente en edades avanzadas el principal impedimento para la inclusión. Se realizó un seguimiento diario de las notificaciones, recibiéndose un total de 364 respuestas. A partir de las consideradas alarmantes y de los valores fuera de rango, se procedió al seguimiento activo y/o contacto telefónico, proporcionando atención farmacéutica adaptada al problema de salud detectado en función de las necesidades.
ConclusionesEl proyecto piloto de Telemedicina TELEA-Farmacia permitió testar la herramienta en pacientes oncológicos en vida real, facilitando el seguimiento continuado, la detección temprana de problemas relacionados con medicamentos y la identificación de nuevas necesidades y puntos de mejora para su implantación definitiva en la actividad asistencial. Para ello, fue necesario compaginar la actividad presencial en consulta con el tiempo requerido para la estratificación y seguimiento telemático. Además, ha evidenciado la necesidad de disponer de nuevos modelos de estratificación en un servicio de farmacia de hospital para la atención farmacéutica que contemplen el manejo de las tecnologías por parte de los pacientes, para identificar así a quienes más se puedan beneficiar de la herramienta de Telemedicina TELEA.
The public health crisis caused by the SARS-CoV-2 pandemic required the adaptation of hospital pharmacy care models to ensure the continuity of follow-up and the safety of patients, without prejudice to health outcomes1,2. Telepharmacy, understood as “remote pharmacy practice based on the use of information and communication technologies (ICT)”, was incorporated by the Spanish Society of Hospital Pharmacy (SEFH) as a strategic healthcare program in the context of the MAPEX program (strategic outpatient pharmaceutical care plan). Telepharmacy has yielded positive results in terms of pharmacotherapeutic follow-up, coordination of multidisciplinary teams, and dispensation/informed delivery of medicines3,4. There is a growing demand for the provision of healthcare services at home, which is facilitated by cutting-edge technologies.
Prior to the outbreak of the pandemic, the Servizo Galego de Saúde (SERGAS) developed a Telemedicine platform called “TELEA” for the follow-up of chronic patients. This ICT-based Telemedicine platform allows communication between health professionals and patients. It is useful for monitoring the health status of patients at home, thereby avoiding travels to the hospital. TELEA is intended to improve the quality of life of patients through close remote follow-up, and facilitate early detection of unbalances in health indicators5.
The Unit of Oncology Pharmacy incorporated this tool to offer telepharmaceutical care to adult patients with cancer. The usefulness of the tool was initially tested in a pilot study called TELEA-Farmacia, which was designed to detect needs and points for improvement of the platform in a small sample of patients. This pilot study was conducted in cancer patients due to the complexity of these cases, since their treatment involves a broad variety of drugs, drug-to-drug interactions, adverse events, and psychosocial problems6. The increasing use of oral antineoplastic agents and improved survival rates make Telepharmacy necessary. Telepharmacy offers advantages both, for patients and health systems, avoids travels, reduces wait times, facilitates pharmacotherapeutic follow-up, improves communication and healthcare quality, enhances patient satisfaction, and involves significant cost-savings7. If these services are complemented with the informed dispensation of medicines, benefits increase8,9.
The main objective of this study was to describe the implementation of the pilot project TELEA-Farmacia and analyze the results obtained to identify opportunities for improvement. Secondary objectives included analyzing platform adherence and evaluating the health status and satisfaction of patients with Telemedicine.
MethodsAn observational, prospective, single-center study conducted between October and December 2021 to implement the pilot project TELEA-Farmacia at the Unit of Oncology Pharmacy of the Service of Hospital Pharmacy of Santiago de Compostela, Spain.
Incorporation of the Pharmacy profile in the TELEA systemPrior to the initiation of the pilot project, a specific pharmacy profile was created on TELEA to include all indicators that reflect the health status of outpatients on follow-up by the Hospital Pharmacy. To such purpose, needs and goals were analyzed, and biological measurements and questionnaires were collected. Then, a regional working group was established including professionals involved in the development and implementation of TELEA. The working group adapted and incorporated these indicators onto the Telemedicine platform TELEA. On this platform, health professionals record health indicators in a remote, safe and integrated way with other hospital information systems.
Patient selection and inclusionBetween October and December 2021, the working group reviewed the medical histories of patients receiving oral antineoplastic agents at the Oncology Pharmacy before a face-to-face consultation. Patients were stratified using the “Stratification and pharmaceutical care model for oncohematologic patients” of the MAPEX project developed by the SEFH10. This model helps prioritize and adjust pharmacy care through the categorization of patients based on demographic, clinical, social, therapeutic, resource, functional, and cognitive variables. According to the score obtained, patients were classified into three levels of priority: priority 1 (high-priority patients, who have a higher overall risk), priority 2, and priority 310.
Candidates for inclusion in the TELEA-Farmacia program were patients with priority 1-2 for receiving pharmaceutical care, and patients who, at pharmacist's opinion, could benefit from Telepharmacy. Patients were required to meet all inclusion criteria and none of the exclusion criteria:
Inclusion criteria:
- •
Age ≥ 18 years.
- •
Diagnosis of a chronic disease and treatment with at least an oral agent that requires hospital dispensation.
- •
Access to ICT by the patient or a relative (availability of at least a mobile phone, tablet or computer).
- •
At least user-level knowledge of the tools required for Telepharmacy, or availability of a caregiver who can help them use the tools and record/submit information.
- •
Availability of the devices necessary to make biological measurements: body temperature, blood pressure, and weight.
- •
Belonging to the healthcare district.
- •
Agreeing to participate in the program and signing an informed consent form.
Exclusion criteria:
- •
Not having access to ICT.
- •
Lacking the skills necessary to use Telepharmacy tools.
- •
Unavailability of devices for making biological measurements.
To access TELEA, patients were asked to install the SERGAS-MÓBIL app or use a web browser. In compliance with personal data protection laws and regulations11, access to the app needed two-step identification requiring a user-password followed by a verification code received by SMS, or a digital certificate (Append Figure 1).
The TELEA platform enables patients to record their biological measurements on a daily, weekly or monthly basis and answer questionnaires adapted to their profile, in this case, a pharmacy profile (Figure 1A). On this platform, the patient selects the questionnaire or biological measurement he or she want to record, and enters the values and/or answers (Figures 1B y 1C, y Append Figures 2 and 3), which are automatically sent to the TELEA version for professionals, which is accessed through the SERGAS medical history (Append Figures 4, 5 and 6).

Table 1 shows biological measurements, periodicity, measurement conditions, therapeutic targets and alerts. Questionnaires included the Spanish version of the questionnaire on quality of life “Patient Reported Outcomes version of the Common Terminology Criteria for Adverse Events” (PRO-CTCAE®)12, and both Visual Analogue Scale (VAS) of pain13 and adherence14. Patients were asked to answer the questionnaire on quality of life once monthly, whereas questionnaires on pain and adherence were completed once weekly. An alert system was not available for these questionnaires, and out-of-range values (occurrence of pain, nausea, vomits, constipation, diarrhea, fatigue …) must be identified by the pharmacist.
Biological measurements on the Telepharmacy platform TELEA-Farmacia
| Biological measurements | |
|---|---|
| Body temperature | |
| Periodicity | Once weekly or when feeling bad (between 07:00 and 12:00 h) |
| Conditions | Axillary temperature |
| Control targets | 35.5-37.5 °C |
| Alerts | Yellow 37.5-37.9 °C; Red: ≥ 38 °C |
| Weight | |
| Periodicity | Once weekly (before breakfast between 07:00 and 12:00 h) |
| Conditions | Always using the same scale (digital, whenever possible) |
| Control targets | BMI: 18.5-24.9. Involuntary weight loss within the last 3-6 months ≤ 5%*. Automatic BMI estimation after the height of the patient is entered, which will be done just once |
| Alerts | Yellow: Involuntary weight loss within the last 3-6 months 5-10% Red: Involuntary weight loss within the last 3-6 months ≥ 10% |
| Blood pressure | |
| Periodicity | Weekly or daily. Self-measurement (between 07:00 and 11:00 h) |
| Conditions | Three separate measurements at 1-2 min intervals. Repeat only when there is a difference of ≥ 10 mmHg between the first two measurements. Blood pressure is the mean of the two last meas-urements |
| Control targets |
|
| Alerts |
|
BMI: body mass index; DBP: diastolic blood pressure; SBP: systolic blood pressure.
Prior to inclusion in the platform, informed consent was obtained, and the telephone number of the patient and/or caregiver was recorded for subsequent identification. First access was performed at the Hospital Pharmacy, where the pharmacist explained to the patient how to use the app, helped him/her score health indicators, and solved questions and doubts. An information leaflet was given to the patient (Append Figure 7) containing instructions for access and a telephone number to contact the unit.
Upon completion of the pilot test, a satisfaction survey (Appen Table 1) was distributed among the patients who had scored more than 25% of indicators. This survey polls their opinion about the simplicity of use, validity to reflect their health status, usefulness, potential points for improvement, and overall level of satisfaction. A five-point Likert scale was used to reflect the level of conformity/satisfaction, ranging from “Not at all satisfied” to “Very satisfied”. With regard to limitations of TELEA-Farmacia, multiple choice was offered, including: easy access to the platform, use of reminders, more adaptable questionnaires, easy submission/receipt of messages, and use of video calls, to name a few.
Satisfaction survey distributed among the patients included in the pilot study TELEA-Farmacia
| 1. Is this the first time you use an information technology (IT) tool for health professionals to monitor your health status? (please, mark an option) |
| YES |
| NO |
| 2. Did you find it easy to use TELEA-Farmacia? (please, mark an option) |
| Extremely difficult |
| Very difficult |
| Neither easy, nor difficult |
| Easy |
| Very easy |
| 3. Do you think that the biological measurements (weight, temperature, blood pressure …) and questionnaires (pain, quality of life, treatment adherence) uploaded by the pharmacist accurately reflect your health status? (please, mark an option) |
| They do not reflect how I feel or my health status at all |
| They do not reflect how I feel or my health status |
| They partially reflect how I feel or my health status |
| They reflect how I feel or my health status |
| They clearly reflect how I feel or my health status |
| 4. Did you find this new communication channel with the Oncology Pharmacy useful? (please, mark an option) |
| No, it did not improve communication with Oncology Pharmacy |
| No, it barely improved communication with Oncology Pharmacy |
| It complements communication with Oncology Pharmacy |
| It improves communication with Oncology Pharmacy |
| It complements and improves communication with Oncology Pharmacy |
| 5. What do you think could be the most important improvement points of the tool? (mark the options you consider necessary) |
| Easy accessibility |
| Create reminders |
| Questionnaires adapted to each health problem |
| Easy submission and receipt of messages to and from the Oncology Pharmacy. |
| New communication channels (video calls) |
| 6. Which is your level of satisfaction with your participation in the TELEA-Farmacia project? (please, mark an option) |
| Not satisfied at all |
| Not satisfied |
| Moderately satisfied |
| Satisfied |
| Extremely satisfied |
In the pilot study, 29 patients were included in TELEA-Farmacia. During this period, the mean number of patients attended at the Oncology Pharmacy was 35 per day, a volume that increased some days. The pharmacist spent 2-3 hours daily reviewing medical histories and performing patient stratification.
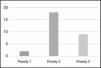
Figure 2 shows the number of patients allocated to each stratification group of the MAPEX model. The most numerous group was the priority-2 group, followed by priority 3. These are patients that, at pharmacist's judgments, could benefit from using the TELEA-Farmacia platform.

The mean age of patients was 59 years (44-75), and 48% were male. With regard to cancer diagnosis, most patients had breast cancer, followed by renal cancer, as shown in Figure 3. The antineoplastic agents most frequently prescribed were cabozantinib (14%), abemaciclib (14%), capecitabine (14%), abiraterone (7%) and pazopanib (7%), among others.

Notifications were reviewed on a daily basis. A total of 364 records of biological measurements and questionnaires were returned. The mean duration of follow-up was 10 (5-13) weeks. In relation to adherence to the use of the platform, the percentage of returned questionnaires was 44%. In general terms, based on the biological measurements and questionnaires returned, patients exhibited a good general health status. When outliers in biological measurements and alarming answers to the questionnaire were identified, active follow-up and/or telephonic contacts were performed. Pharmaceutical care was adapted to the health problem detected according to the needs of each patient.
Concerning the satisfaction survey, for 14 of the patients who completed their questionnaires, this was the first time they used a health monitoring tool. According to the responses received, TELEA was considered easy-to-use (7% “very easy”; 57% “easy”; 36% “neither easy nor difficult”) and “useful” (22% considered that “it notably complements and improves communication with the Oncology Pharmacy”; 64% considered that “it improves communication”; 14% considered that “it complements communication”). Respondents considered that the health indicators included were appropriate (79% reflect how they feel and their health status, 21% partially reflect how they feel and their health status). The main limitations found were difficulty accessing the platform (which led us to design an information leaflet), and the absence of reminders of pending questionnaires. Patients also suggested incorporating the use of video calls. Overall satisfaction was good (14% were “very satisfied”; 86% were “satisfied”).
DiscussionTELEA-Farmacia emerges as the first digital Telepharmacy platform used in Hospital Pharmacy in Galicia. The purpose of this pilot project was to analyze the use of the platform by cancer patients attended at the Oncology Pharmacy, and identify needs, limitations and points for improvement prior to its incorporation into routine practice.
In general terms, TELEA-Farmacia facilitated follow-up, biological measurements, and the evaluation of health outcomes in patients attended in the Oncology Pharmacy consultation, remotely and in real time. This project required patient engagement, which favored self-care and their empowerment, leading patients to adopt an active role in the management of their disease. TELEA-Farmacia is postulated as a potential tool that favors continuous follow-up through close communication, thereby facilitating early telepharmaceutical care, adapted to the individual needs of each patient. Notably, this pilot project has also facilitated the identification of improvement points that will help us optimize the model prior to its incorporation into routine practice.
The working group selected TELEA due to its advanced level of development and availability. The usefulness of this tool for Telemedicine had been previously demonstrated in the follow-up of patients with COVID-19, carriers of implanted heart devices, and patients with chronic diseases such as heart failure or diabetes5,15. As this tool was developed by SERGAS, personal data protection is guaranteed, with ensures the safety, privacy and confidentiality of data. Another advantage is that TELEA is fully integrated with hospital information systems, which ensures interoperativity and information sharing. These two characteristics are important for the validation of Telepharmacy tools recommended by MAPEX panels16.
For TELEA to be implemented, it was necessary that a specialist pharmacist was involved and combined the review of medical histories, patient stratification, inclusion, and subsequent follow-up of patients with the daily consultations. When the number of appointments was high, face-to-face consultations were prioritized over teleconsultation. The workload limited inclusion, since it is necessary that wait times are short to create a favorable mood for patients to agree to participate in the project. Therefore, it is necessary that enough personnel and time are available for teleconsultations, in order to be able to continue the inclusion and follow-up of patients using Telepharmacy services.
The advanced age of many of the patients with higher scores on the stratification model was another limitation to inclusion in the platform. Thus, most patients did not have ICT and/or enough digital skills. This difficulty makes it necessary to employ other prioritization models that consider the use of ICT and digital skills of patients. This will facilitate the identification and selection of patients who can benefit from telepharmaceutical care. The SEFH has made recent progress through the publication of a new stratification model in Telepharmacy that considers these aspects, along with factors related to home dispensation17–19. However, this document was published after this pilot project was initiated.
With regard to the diseases of the patients included, the high percentage of patients with breast cancer may be due to the fact that they are young, proactive patients involved in the management of their disease and treatment, which may have favored their inclusion. In addition, some drugs such as abemaciclib or capecitabine are associated with the occurrence of adverse events that can be easily monitored with TELEA, such as diarrhea, which makes telemonitoring profitable. This helped us identify another point for improvement: the incorporation of questionnaires adapted to the type of expected adverse reactions that reflect the health status of the patient. These questionnaires would include questions such as the number of daily bowel movements, days with diarrhea, and number of capsules of loperamide necessary to counter this side event.
The two-step identification system was another difficulty found by patients, as it made access to the platform more difficult. However, this identification system guarantees confidentiality and data protection. Patients also claimed to need reminders, which was determined as an important improvement point. Thus, an alternative alarm system is necessary to remind patients that they have to answer questionnaires within the established deadlines. These two factors probably explain the poor adherence to the tool, demonstrated by the low number of questionnaires returned with respect to the expected number of questionnaires. Therefore, the most important and urgent points for improvement were that the identification process have to be simplified and reminders of pending questionnaires have to be created. Nevertheless, the platform reflected the good health status of the patients included in the project, which favored active follow-up and/or telephonic contact in case alarming responses were detected.
Along with meeting the needs detected in the pilot project, the following step is to coordinate Telepharmacy with remote dispensation and informed delivery of medicines, combined with face-to-face consultations. This advancement will improve flexibility in the dispensation and delivery of medicines, which will reduce travels to the hospital and patient's dependence on the health center, also resulting in a reduction of wait times at the hospital pharmacy. TELEA also will help optimize workloads and schedule face-to-face consultations when they are really necessary, which helps humanize healthcare by focusing it on the real needs of patients.
The pilot project TELEA-Farmacia allowed us to test the tool in cancer patients in a real-life context, facilitated continuous follow-up, the detection of drug-related events, and early intervention adapted to the health problems of each patient. This experience helped us identify unknown needs of patients and health professionals, and detect points for improvement prior to the incorporation of this tool in the Hospital Pharmacy Service. The use of Telemedicine platforms requires that enough personnel and time are available to combine face-to-face consultations with patient stratification, inclusion, and remote follow-up. This pilot project revealed that new prioritization models are necessary in Hospital Pharmacy that consider the digital skills of patients and help identify those who will benefit from Telepharmacy.
FundingNo funding
Conflict of interestsNo conflicts of interest
Contribution to the scientific literature
There is a growing demand for healthcare services at home, which is made possible by advances in information and communication technologies.
We describe the implementation and results of a pilot project of Telepharmacy for cancer patients. The patients included in the study were asked to use a mobile app to regularly record their biological measurements and quality-of-life questionnaires. The active follow-up of responses from the Oncology Pharmacy consultation allowed the pharmacist to provide pharmaceutical care adapted to the health problem detected.








