








To analyze the impact of introducing omeprazole in the drug formulary of the Hospital de Barbanza on prescriptions made in hospital and out-of-hospital (Outpatient Units and Primary Care) for all Proton Pump Inhibitors (PPIs).
Material and methodsA 36-month retrospective descriptive study in a level I hospital. The basic units of work are Dose-Population-Day in the outpatient setting, and the Defined Daily Dose/stays-day for hospitalized patients; the proportion of DDDs for omeprazole vs. the rest of PPIs is used as measure of efficiency. For statistical analysis, we built a segmented regression model.
ResultsIn the outpatient units, there are statistically significant changes for pantoprazole and rabeprazole. The first drug, which was stable before the intervention, suffered an immediate decrease; rabeprazole, which was increasing before the intervention, presented a subsequent downward trend. In Primary Care, a statistically significant change was confirmed for pantoprazole, with a long-term decreasing trend. In hospitalization, statistically significant changes were observed for pantoprazole and omeprazole; the first one with an immediate decrease and a long-term tendency to decrease, while omeprazole experienced an immediate increase and long-term growth. The evolution of the omeprazole percentage vs. all PPIs showed increases in all three scenarios.
ConclusionsA shift to a more efficient prescription of PPIs was observed in all healthcare settings following the introduction of omeprazole in the hospital drug formulary. The inclusion of efficient drugs, or the removal of those Inefficient, can be a potentially useful tool In order to Improve prescription profiles.
Analizar el impacto de introducir el omeprazol en el formulario del Hospital de Barbanza sobre las prescripciones intrahospitalarias y extrahospitalarias (consultas externas y atención primaria) de todos los Inhibidores de la Bomba de Protones (IBP).
Material y métodosEstudio descriptivo retrospectivo de 36 meses en un hospital de nivel I. Las unidades básicas de trabajo son las dosis-habitantes-día en el ámbito extrahospitalario y las dosis diarias definidas/estancias-día para hospitalización; como medida de eficiencia se utiliza el porcentaje de DDD de omeprazol sobre el resto de IBP. Para el análisis estadístico construimos un modelo de regresión segmentada.
ResultadosEn consultas externas sufren cambios estadísticamente significativos el pantoprazol y el rabeprazol; el primero, estacionado antes de la intervención, sufre una disminución inmediata; el rabeprazol, en crecimiento antes de la intervención, presenta una posterior tendencia decreciente. En atención primaria se constata un cambio estadísticamente significativo en el pantoprazol, con tendencia decreciente a largo plazo. En hospitalización se observan cambios estadísticamente significativos para el pantoprazol y el omeprazol; el primero con disminución inmediata y tendencia al decrecimiento a largo plazo; el segundo experimenta un aumento inmediato y crecimiento a largo plazo. La evolución del % de omeprazol respecto al total de IBP mostró aumentos en los tres escenarios. Conclusiones: Se observa un cambio hacia una prescripción de IBP más eficiente en todos los ámbitos asistenciales tras la introducción del omeprazol en la guía farmacoterapéutica del hospital. La Inclusión de medicamentos eficientes, o la retirada de Ineficientes, puede ser una herramienta potenclalmente útil para mejorar los perfiles de prescripción.
The present article analyzes the effect on prescription by the inclusion of a new medication in the formulary of a hospital, regarding all drugs in the same therapeutic group; its scope is differentiated within 3 patient care levels: hospitalization (hospitalized patients), outpatient units (patients from hospital outpatient units) and Primary Care centres of referral (outpatients managed at their health centre).
This research intends to show the shift and evolution in the use of the whole group of Proton Pump Inhibitors as a consequence of the inclusion of omeprazole in the hospital formulary, and to verify if this behaviour is useful or in line for achieving a more efficient prescription.
We consider that this is a matter of high interest due to its novelty, given that no study in Spain has conducted any research about this effect, and therefore there is no scientific evidence at all about the consequences of the inclusion in the formulary of a new medication upon the use of the rest of the drugs in the same therapeutic group in our country, not only in the hospital setting, but also in the setting of hospital outpatient units and in Primary Care centres with the same hospital of reference where the intervention has been conducted.
IntroductionThe hospital formulary is the list of all those drugs selected by the Pharmacy Committee from a specific hospital, that are available to be used in hospitalized patients; it is a measure for rational use by the National Health System. Some areas in the Primary Care setting have used this type of tool; however, these are presented as recommendations, and there is complete freedom for prescription outside it1, even though some countries enforce its use in this level of care2-3.
At the time of selecting the medications to be included in the formulary, the rule will be not considering the retail pharmacy price for said drugs4; however, it has been confirmed that there is a direct effect on the subsequent use of those medications after hospital discharge4. In countries other than Spain, it has been detected that hospital prescription will have an influence on Primary Care 5-6, which seems to have a direct association with hospital discharge reports and prescriptions at Outpatient Units7. Other studies have assessed the influence of a change in the formulary upon out-of-hospital prescriptions4, but none has been conducted in Spain.
In our country, pharmaceutical expenses have reached in recent years around 10,000 million euros per year at outpatient level8 and around 4,000 million at hospital level, which will became over 6,000 million in 2015 if the new due to the inclusion of the new drug therapies against the Hep hepatitis C virus are included9. These issues lead to conduct a specific monitoring of the evolution in pharmaceutical services provided by the Galician Health System (SERGAS), as well as by other Autonomous Communities. And one of the indicators used to determine prescription efficiency is the Proportion of Omeprazole over the rest of Proton Pump Inhibitors (PPIs), because this is considered the IBP of choice due to its superior efficiency. The healthcare areas, or Organizational Structures of Integrated Management (EOXI) from the SERGAS, are the peripheral executive management agencies that integrate Primary Care and Hospital Care10.
Considering a Health System that consists of two levels of care, it seems essential that, at the time of selecting a medication to be included in the hospital formulary, its price and its potential impact on the outpatient setting should also be taken into account. This aspect is particularly relevant when this inclusion is considered only due to the price reductions negotiated within the hospital, because this could represent an additional cost if the overall balance is damaging for the Health System as a whole.
On June, 2014, the omeprazole molecule was included in the formulary of the Hospital de Barbanza (Galicia, Spain); so far, only pantoprazole and esomeprazole were available in the formulary (the latter was restricted for patients with a nasogastric tube). At that time, the cost in Spain of an omeprazole DDD was approximately 10 times lower than the DDD for any other PPI 11.
The objective of our study was to analyze the impact of omeprazole introduction in the formulary of the Hospital A Barbanza on hospital (hospitalization) and out-of-hos- pital prescriptions (outpatient units and Primary Care), in the overall Proton Pump Inhibitor therapeutic group.
MethodologyIn Spain, the public healthcare insurance implemented covers practically the whole population. The present research paper is focused on a hospital from the SERGAS network; namely a Level I regional hospital12 located in the town of Ribeira within the A Coruna province, with an assigned population of 64,287 inhabitants in 2014, and 64,655 in 2015, and four Primary Care centres of referral: A Pobra de Caramihal (9,186 inhabitants), Boiro (18,925 inhabitants), Porto do Son (8,692 inhabitants) and Ribeira (27,852 inhabitants). With 81 beds, the evolution of its occupancy rate has been of 86.16% in 2013, 80.80% in 2014 and 81.92% in 201 5.
The Defined Daily Doses (DDDs) for each PPI were the basic work units; these allowed us to analyze the monthly time sequences of use of each molecule evaluated. It is defined as the assumed mean daily dose of a medication, when used for its main indication. DDDs, according to the anatomical classification of medications13, are in continuous review by the WHO14. The following DDD equivalences were determined: omeprazole (DDD 20 mg), pantoprazole (DDD 40 mg), lansoprazole (DDD 30 mg), rabeprazole (DDD 20 mg) and esomeprazole (DDD 30 mg), both for oral and parenteral formulations.
The use of DDDs allows us to conduct comparative studies of use, regardless of variations in price and in the weight contents of each pharmaceutical form. Generally, the number of DDDs used in an area or centre is expressed, in descriptive studies, per 1,000 inhabitants and per day: this is called the Day Inhabitant Dose (DID). This parameter offers an approximate volume of the population treated daily with the normal dose of a specific drug, and therefore its use allows to expose any differences in therapy practices.
In the outpatient setting, the mean use is expressed in DIDs, as already mentioned; this measure will be used for the analysis in Outpatient Units and Primary Care. However, DDD per 100 hospital stays and day15 (DDD/ stays-day) will be used for calculating the use in hospital for in-patients, and this will provide an estimate of the likelihood for a patient to be treated with a specific medication during hospital stay, or in other words, the proportion of hospitalized patients treated with a specific drug during their hospitalization. These two units, DID and DDD/stays-day, are the ones we have used for statistical calculation.
We have differentiated three forms of care (Outpatient Units, Primary Care, and Hospitalization), and in all of them, the efficiency measure used has been the percentage or proportion of omeprazole DDD over the total DDD of all PPIs prescribed; we represent this as: %DDDomeprazole/DDDtotalPPI.
Regarding the timeframe, a descriptive study was conducted during 36 months, from January, 2013 to
December, 2015. The change in the hospital formulary by the inclusion of the omeprazole molecule was implemented on June, 6th, 2014; and therefore this analysis covers a similar period before and after the intervention.
Data regarding dispensing and acquisitions charged against the SERGAS were obtained from the official corporate information systems:
- a.
All dispensing conducted by the community pharmacies in the healthcare area linked with the prescriptions conducted by physicians from any of the four Primary Care services in the area of referral by the hospital and its outpatient units.
The information was obtained from the Pharmacy Service Information System, as number of packages dispensed each month, transformed into DDD per month, and subsequently into monthly DIDs.
- b.
Of all dispensing conducted by the Pharmacy Unit in the Hospital A Barbanza, using the Pharmacy Service Information System database, which provides the number of packages used, transformed into DDD per month, and subsequently into DDD/stays-day.
For statistical analysis, we built a segmented regression model of interrupted time series16. The intervention studied was the inclusion of the omeprazole molecule in the formulary of the previously mentioned hospital.
In this analysis, the dependent variable was DID or DDD/stays-day, or the %DDDomeprazole/DDDtotalPPI of the different PPIs per month; and the independent variables were:
- -
Time from the start of the study, which shows the time trend previous to the change in the hospital formulary (or intervention).
- -
A binary variable that takes the value of 0 before and of 1 after the change in the formulary, which would show the immediate change after the intervention.
- -
A time variable since the change in the formulary, which took the value of 0 before the intervention, and afterwards the values of 1,2,3… that would show the change in trend at long term.
The segmented regression model will conduct 2 regression lines, one with data before the change in the formulary, and the other with subsequent results data after the change in the formulary :.As result it provides 4 coefficients (when DID is mentioned, it can be extrapolated to DDD/stays-day or %DDDomeprazole/DDDto- talPPI):
- 1.
Intercept. It is the cut-off point of the first line with the Y axe; it represents the value of DID estimated by regression method at the start of the study. If the coefficient was not statistically significant (SS), the conclusion could be that the value of DID was not different from zero at the start of the period of study.
- 2.
Trend previous to the change in the formulary. It is the slope of the first line; it represents the increase or decrease value in DID values before the change. If the coefficient was not SS, the conclusion could be that there was neither increase nor decrease before the change. If the coefficient was positive and SS, the conclusion could be that DIDs were increasing before the intervention; and if the coefficient was negative, that DIDs were decreasing before the change.
- 3.
Immediate impact of the change in the formulary. This is the difference between the end of the first line and the beginning of the second line; it represents the leap or immediate reduction in DID values. If the coefficient was not statistically significant, the conclusion could be that there was no leap or immediate reduction in values. If the coefficient was positive and SS, the conclusion could be that DIDs have experienced an immediate leap, and if it was negative, that DIDs have experienced an immediate reduction.
- 4.
Change in trend after the change in the formulary. This is the difference between the slope in the second line and the slope in the first one, which represents the likely change in increase or decrease at long-term in DID values that could have occurred after the intervention regarding the increase or decrease rate before the change. If the coefficient was not SS, the conclusion could be that there has been no modification in the decrease or increase at long term in their values. If the coefficient was positive and SS, the conclusion could be that, after the change in the formulary, DIDs have started increasing at a faster rate (if they were increasing or stable before the intervention) or decrease at a lower rate (if they were decreasing or stable before the change).
As measure for statistical model adjustment, we used the R2 value.
ResultsFirst setting: Outpatient UnitsFigure 1 shows the evolution over time of the DIDs for the different PPIs for medical prescriptions conducted for outpatient dispensing by hospital physicians; it stands out that the DIDs for pantoprazole experienced a first sharp decrease and subsequently showed a slight increasing trend.

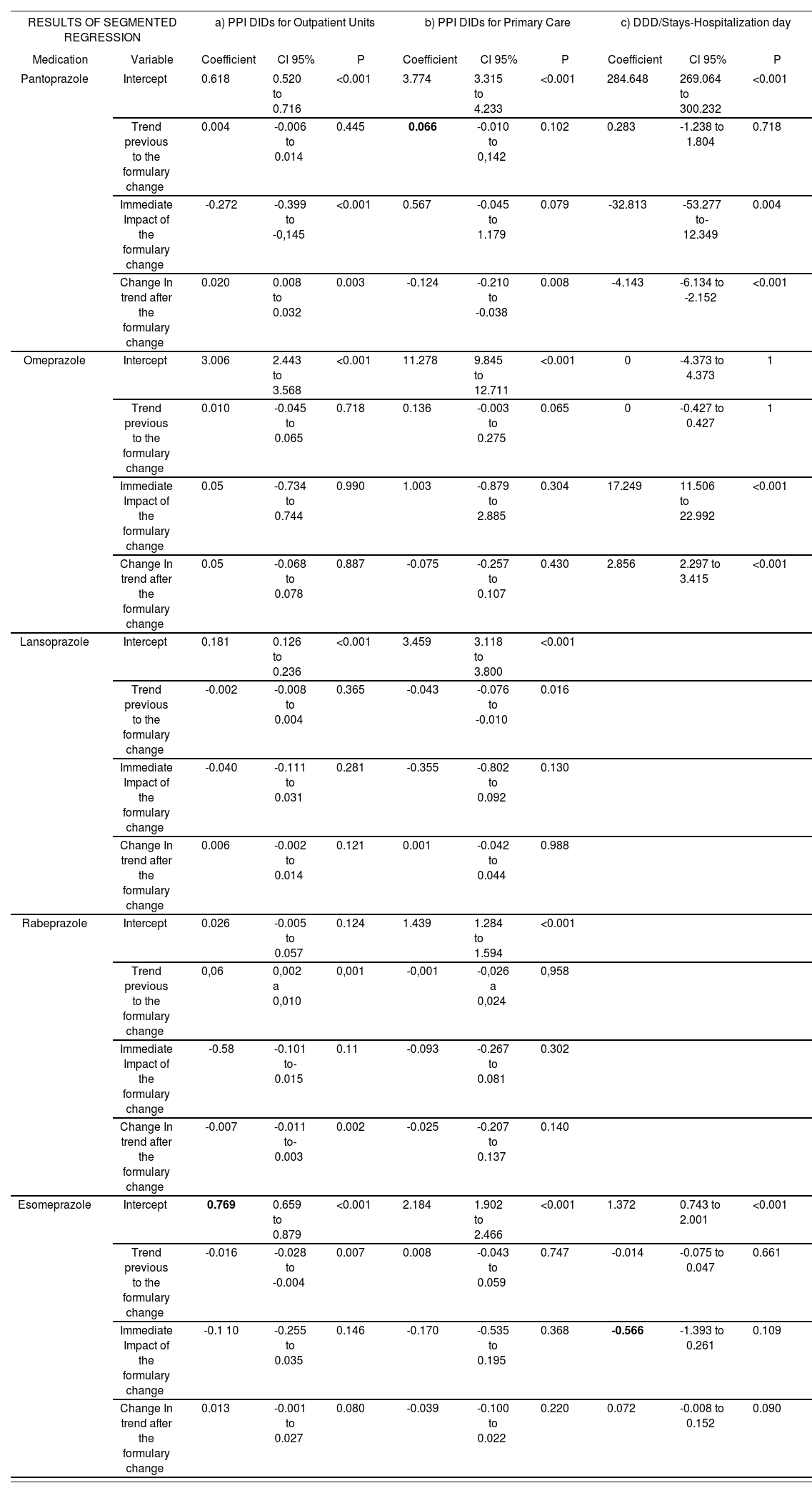
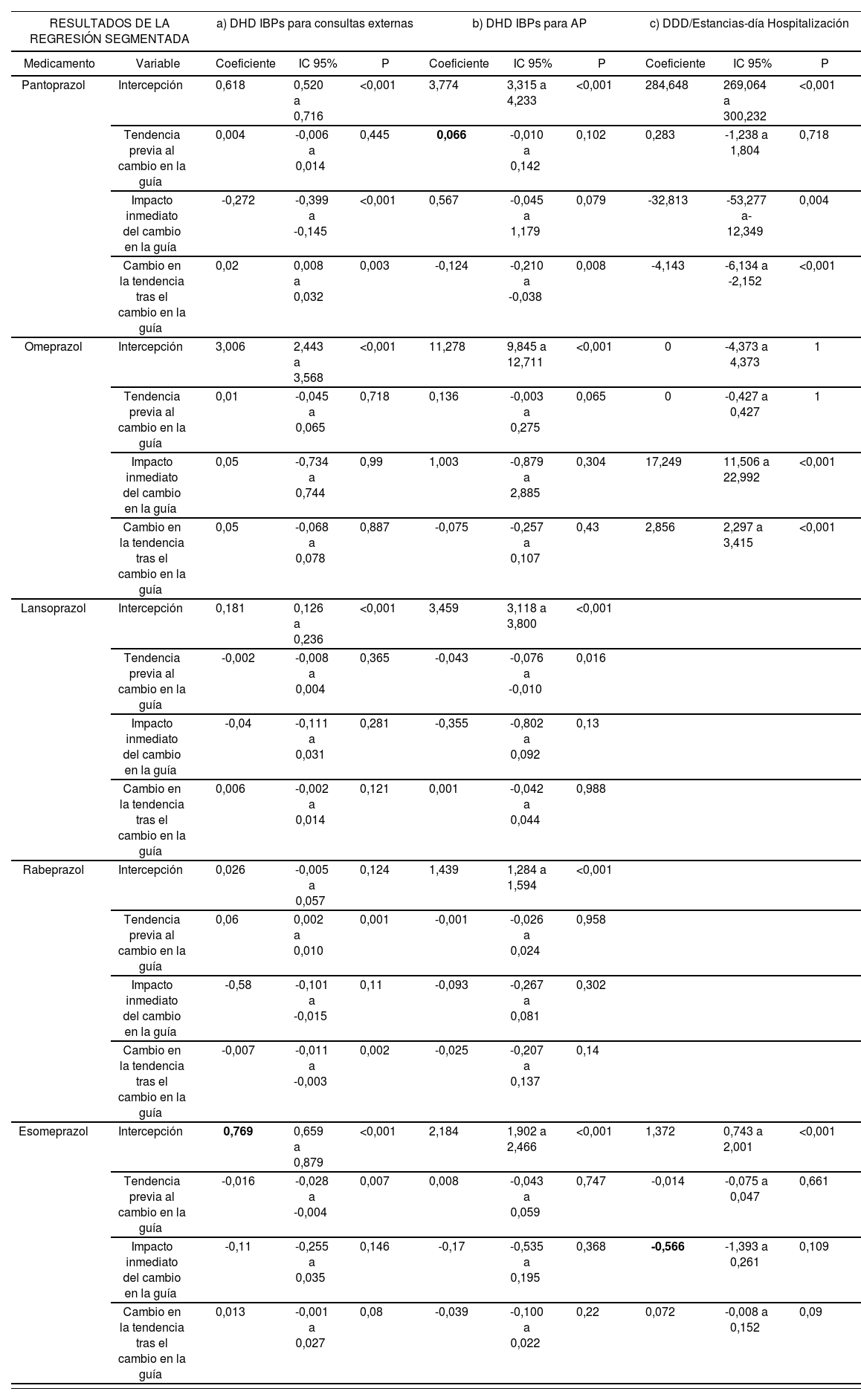
Segmented regression of DID data for the different PPIs in Outpatient Units showed a mean R2 of 0.346. Its results (Table 1.a) show that the use of pantoprazole was stationary before the change in the formulary, and experienced a sharp SS decrease afterwards, followed by a slight increase at long-term, also significant. The use of rabeprazole before the change showed a SS increase, and did not experience an immediate change after the intervention, although its subsequent trend at long-term presents a significant decrease. Esomeprazole, which showed a significant reduction in its use before the change, did not show any SS changes. The remaining PPIs (omeprazole and lansoprazole) did not show SS values for the trend previous or after the change in the formulary.
Results of the segmented regression analysis for the three settings studied, from January, 2013 to December, 2015.
| RESULTS OF SEGMENTED REGRESSION | a) PPI DIDs for Outpatient Units | b) PPI DIDs for Primary Care | c) DDD/Stays-Hospitalization day | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Medication | Variable | Coefficient | Cl 95% | P | Coefficient | Cl 95% | P | Coefficient | Cl 95% | P |
| Pantoprazole | Intercept | 0.618 | 0.520 to 0.716 | <0.001 | 3.774 | 3.315 to 4.233 | <0.001 | 284.648 | 269.064 to 300.232 | <0.001 |
| Trend previous to the formulary change | 0.004 | -0.006 to 0.014 | 0.445 | 0.066 | -0.010 to 0,142 | 0.102 | 0.283 | -1.238 to 1.804 | 0.718 | |
| Immediate Impact of the formulary change | -0.272 | -0.399 to -0,145 | <0.001 | 0.567 | -0.045 to 1.179 | 0.079 | -32.813 | -53.277 to-12.349 | 0.004 | |
| Change In trend after the formulary change | 0.020 | 0.008 to 0.032 | 0.003 | -0.124 | -0.210 to -0.038 | 0.008 | -4.143 | -6.134 to -2.152 | <0.001 | |
| Omeprazole | Intercept | 3.006 | 2.443 to 3.568 | <0.001 | 11.278 | 9.845 to 12.711 | <0.001 | 0 | -4.373 to 4.373 | 1 |
| Trend previous to the formulary change | 0.010 | -0.045 to 0.065 | 0.718 | 0.136 | -0.003 to 0.275 | 0.065 | 0 | -0.427 to 0.427 | 1 | |
| Immediate Impact of the formulary change | 0.05 | -0.734 to 0.744 | 0.990 | 1.003 | -0.879 to 2.885 | 0.304 | 17.249 | 11.506 to 22.992 | <0.001 | |
| Change In trend after the formulary change | 0.05 | -0.068 to 0.078 | 0.887 | -0.075 | -0.257 to 0.107 | 0.430 | 2.856 | 2.297 to 3.415 | <0.001 | |
| Lansoprazole | Intercept | 0.181 | 0.126 to 0.236 | <0.001 | 3.459 | 3.118 to 3.800 | <0.001 | |||
| Trend previous to the formulary change | -0.002 | -0.008 to 0.004 | 0.365 | -0.043 | -0.076 to -0.010 | 0.016 | ||||
| Immediate Impact of the formulary change | -0.040 | -0.111 to 0.031 | 0.281 | -0.355 | -0.802 to 0.092 | 0.130 | ||||
| Change In trend after the formulary change | 0.006 | -0.002 to 0.014 | 0.121 | 0.001 | -0.042 to 0.044 | 0.988 | ||||
| Rabeprazole | Intercept | 0.026 | -0.005 to 0.057 | 0.124 | 1.439 | 1.284 to 1.594 | <0.001 | |||
| Trend previous to the formulary change | 0,06 | 0,002 a 0,010 | 0,001 | -0,001 | -0,026 a 0,024 | 0,958 | ||||
| Immediate Impact of the formulary change | -0.58 | -0.101 to-0.015 | 0.11 | -0.093 | -0.267 to 0.081 | 0.302 | ||||
| Change In trend after the formulary change | -0.007 | -0.011 to-0.003 | 0.002 | -0.025 | -0.207 to 0.137 | 0.140 | ||||
| Esomeprazole | Intercept | 0.769 | 0.659 to 0.879 | <0.001 | 2.184 | 1.902 to 2.466 | <0.001 | 1.372 | 0.743 to 2.001 | <0.001 |
| Trend previous to the formulary change | -0.016 | -0.028 to -0.004 | 0.007 | 0.008 | -0.043 to 0.059 | 0.747 | -0.014 | -0.075 to 0.047 | 0.661 | |
| Immediate Impact of the formulary change | -0.1 10 | -0.255 to 0.035 | 0.146 | -0.170 | -0.535 to 0.195 | 0.368 | -0.566 | -1.393 to 0.261 | 0.109 | |
| Change In trend after the formulary change | 0.013 | -0.001 to 0.027 | 0.080 | -0.039 | -0.100 to 0.022 | 0.220 | 0.072 | -0.008 to 0.152 | 0.090 | |
Statistically significant if p<0.05
Figure 2 shows the evolution of the DIDs for different PPIs in Primary Care centres for which the Hospital de Barbanza is their referral centre.

Segmented regression of DID data from different PPIs for Primary Care showed a mean R2 of 0.588. Their outcomes (Table 1.b) show that pantoprazole DIDs did not experience any SS increase or decrease before the introduction of omeprazole in the formulary; no change with immediate effect has been observed either. However, there was a change of trend after the intervention: the use of pantoprazole tended to decrease at longer term. Lansoprazole DIDs showed a decreasing trend before the change in the formulary, and afterwards no SS immediate change was perceived, nor any trend modification at long term. The other PPIs did not show any SS trends before the intervention, and no leaps or changes in trend subsequently.
Third setting: HospitalizationIn hospitalization, Figure 3 shows that after the formulary change, the use of pantoprazole at hospital level started to decrease, the use of omeprazole presented an increasing trend, and the use of esomeprazole continued stable.

The segmented regression of DDD/stays-day data showed a mean R2 of 0.660. Its results (Table 1.c) showed that pantoprazole did not present any SS increase or decrease before the change in the formulary, but a statistically significant strong immediate reduction was observed after the intervention, as well as an alteration in the long-term trend regarding the use of pantoprazole which tends to decrease in a SS manner.
In the case of omeprazole, it was observed in a SS way that after its inclusion in the hospital formulary, there was an immediate increase in its use, as well as an increasing trend at long term. For esomeprazole, no previous trend was observed, and no significant change after the formulary modification was observed either.
%DDDomeprazole/DDDtotal PPI in the three settingsRegarding the percentage of the DDD of omeprazole compared with the total DDD for all PPIs, Figure 4 shows that, after the change, there is a clear increasing trend at hospital level, and an immediate leap at Outpatient Unit level, followed by a stable situation. In this last setting, the evolution of the average percentages of DID prescription of this molecule over the rest of PPIs during the period studied was 72.58%, reaching its highest peak on September, 2014 with 86.49% (Figure 4). In the prescriptions at the Primary Care setting, this average percentage was 58.14%, with an increasing evolution during the whole study.

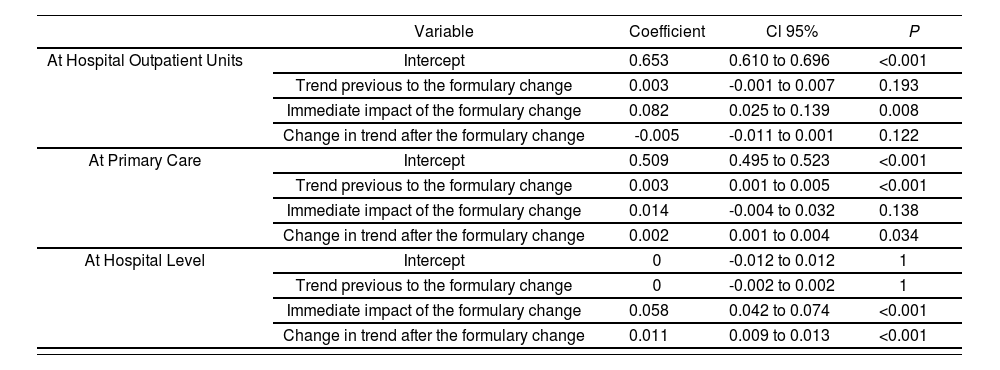
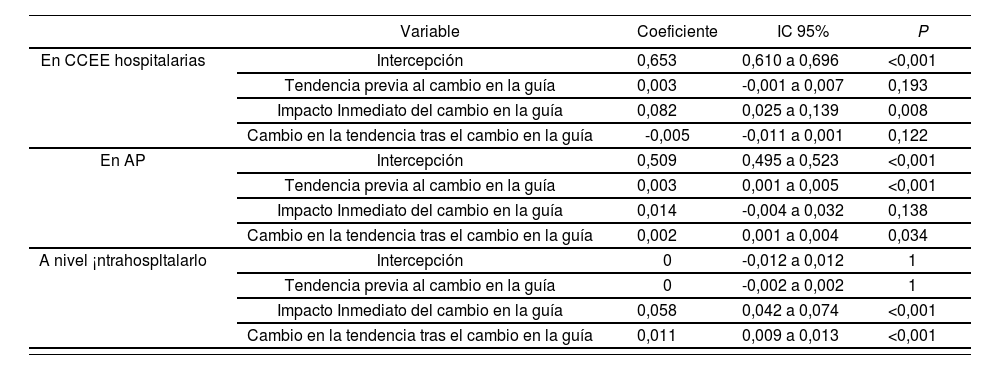
Segmented regression showed a mean R2 of 0.835. Its outcomes (Table 2) showed that after the intervention there was an immediate SS leap at hospital level, and subsequently a SS increasing trend at long-term. In the Outpatient Units, there was an immediate SS leap after the intervention, but the subsequent trend at long term continued stable and was not SS. In Primary Care, the long-term trend before the intervention was alre-ady increasing in a SS manner, and no SS immediate leap was observed; however, there was a SS long-term change in terms of an acceleration of the increasing trend.
Results of the Regression for the variable: DDD proportion of omeprazole over total DDD for PPIs.
| Variable | Coefficient | Cl 95% | P | |
|---|---|---|---|---|
| At Hospital Outpatient Units | Intercept | 0.653 | 0.610 to 0.696 | <0.001 |
| Trend previous to the formulary change | 0.003 | -0.001 to 0.007 | 0.193 | |
| Immediate impact of the formulary change | 0.082 | 0.025 to 0.139 | 0.008 | |
| Change in trend after the formulary change | -0.005 | -0.011 to 0.001 | 0.122 | |
| At Primary Care | Intercept | 0.509 | 0.495 to 0.523 | <0.001 |
| Trend previous to the formulary change | 0.003 | 0.001 to 0.005 | <0.001 | |
| Immediate impact of the formulary change | 0.014 | -0.004 to 0.032 | 0.138 | |
| Change in trend after the formulary change | 0.002 | 0.001 to 0.004 | 0.034 | |
| At Hospital Level | Intercept | 0 | -0.012 to 0.012 | 1 |
| Trend previous to the formulary change | 0 | -0.002 to 0.002 | 1 | |
| Immediate impact of the formulary change | 0.058 | 0.042 to 0.074 | <0.001 | |
| Change in trend after the formulary change | 0.011 | 0.009 to 0.013 | <0.001 |
Statistically significant if p<0.05
In this study, a clear change is observed in PPI prescription after the introduction of omeprazole in the hospital formulary for prescriptions within and outside hospital, particularly for pantoprazole. In the first setting, this change is immediate and marked, with an inmediate increase in the percentage of omeprazole, and with an increasing trend afterwards; in Outpatient Units, an immediate leap in the percentage of omeprazole is observed, but no change in increase trend at long term; and in Primary Care, this percentage does not present an immediate leap, but an increase in the rate of growth after the formulary change.
Regarding the use of each one of the PPIs, at hospital level it was observed that, after the introduction of omeprazole in the formulary, at the same time that there was an increase in the DDD/stays-day for omeprazole, there was a reduction in the ones for pantoprazole, while those for esomeprazole continued stable. The latter can be due to the fact that the use of esomeprazole was already restricted.
At Outpatient Unit level, no change in omeprazole DIDs was observed, but an immediate reduction in the ones for pantoprazole, as well as a change of trend for those of rabeprazole. The change observed in pantoprazole prescriptions might be explained by the shifts in its hospital prescriptions, that will finally end up as prescriptions after discharge; in the case of rabeprazole, its prescription rate is so low (mean DID of 0.067) compared with the rest of PPIs (mean DID for omeprazole: 3.225) that slight changes in the relative prescription for the other PPIs might have had a relative major displacement effect for this drug. The lack of change in omeprazole DIDs can be due to the high number of DDDs previous to the intervention in the formulary in Outpatient Units, compared with the DDDs at hospital level; for example, on June, 2014, 2.947 omeprazole DIDs were used in Hospital Units, and 18.539 DDD/stays-day at hospital level; and if we consider that the hospital has 81 beds and 65,000 inhabitants, we can see that on June, 2014, 364 omeprazole DDDs were prescribed at hospital level, and 5,684 DDDs in Outpatient Units; therefore, the influence that the former can have on the latter is more limited that the influence that DDDs for pantoprazole can have at hospital and out-of-hospital level, where differences are not so marked.
There is no SS change in Primary Care physicians regarding omeprazole; however, there is a change in pantoprazole prescriptions: their DIDs don't show an immediate sharp decrease, but then there is a decreasing trend at long term. The explanation for this could be in the prescription induced from the Outpatient Units towards Primary Care17,18,19-21. No fast change was observed in pantoprazole prescriptions in Primary Care, unlike in Outpatient Units; this could be due to the fact that omeprazole DIDs in Outpatient Units are extremely lower than omeprazole DIDs in Primary Care; specifically, in Outpatient Units, the omeprazole DIDs at June, 2014 were 2.947, and their mean during the study was 3,225, vs. the situation in Primary Care, where DIDs at June, 2014 were 13.647, and the mean DID during the study was 13.934.
Regarding the evolution of the proportion of omeprazole DDD regarding all DDD for PPIs, the study shows that there is an increase in all levels, which is immediate in hospitalization and Outpatient Units, and at longer term in Primary Care. Omeprazole is the PPI of choice, and therefore PPI prescription becomes more efficient in the three settings.
We haven't found any studies assessing what happens in different healthcare settings after the incorporation of a new PPI to the hospital medication formulary, with this approach as a longitudinal analysis of time series. We have located one study about the impact of the change upon the formulary of a hospital on prescriptions, both at hospital discharge and at a time-point some months after hospitalization4, which evaluates withdrawing esomeprazole because its price is ten times higher than that for another PPI, and replacing it by a more efficient PPI. In this study, which analyzed 3 transversal points (before hospital admission, at discharge, and afterwards), it was found that before the change in the formulary, the majority of patients were taking esomeprazole at hospital discharge as well as some months afterwards, while after its withdrawal, its use was residual both at hospital discharge and some months afterwards, and efficient PPIs were most widely used.
We did not find any studies to analyze the effect of the formulary change upon prescription within hospital and out-of-hospital at the same time; we did find studies analyzing the effect of PPIs outside hospital after a change in the formulary; and other studies that found, like ours, that the change in the formulary was associated with changes in the use of the medication at hospital22-23.
Pharmacy service should be managed transversally, because changes in the hospital guidelines will entail changes in prescription patterns. These changes should be assessed when price reductions become the driver for including new medications in the hospital formulary, because of their overall effect24.
Our study is ecologic, and any causality relationship should be interpreted cautiously; however, previous studies have found said association24. Another limitation could be the lack of reference to clinical variables; however, there is sufficient scientific evidence in this case about the fact that no PPIs present an efficacy superior to the rest for their approved clinical indications and if used in equally potent doses25; therefore, no clinical variations should be expected. In terms of safety, there are no apparent differences in adverse effects25.
On the other hand, it is worth mentioning that there has been no assessment of the evolution of the direct costs of medications, because one month after the inclusion of omeprazole in the formulary, there was a reduction in the price of PPIs26, followed by a second one on October, 201 527, and this represents an important confusion factor for the conclusion that any changes in this variable are exclusively a consequence of the intervention.
As a final conclusion, we can state that the inclusion of omeprazole in the hospital formulary has had an influence in PPI prescription patterns, both in hospitalization and in Outpatient Units and Primary Care, and this has led to a more efficient use of these drugs.
The inclusion of efficient medications in the formulary, or the withdrawal of inefficient drugs, can be a potentially useful tool and effective at long-term in order to improve the prescription profiles in all levels of care.
Contributions to AuthorshipRaquel Vázquez Mourelle conceived the present article, and devised the methodological design of the analysis jointly with Eduardo Carracedo Martinez; Raquel Vázquez Mourelle conducted the exploitation, validation and transformation of hospitalization data, while Eduardo Carracedo Martinez did the same with Specialist and Primary Care Centres; both authors were jointly responsible for data analysis and interpretation in the three settings presented. Raquel Vázquez Mourelle was in charge of writing the article, while Eduardo Carracedo Martinez conducted a critical review of the different versions, with major intellectual contributions. Both authors have approved the final version of the manuscript.
FundingNone.
AcknowledgementsNone.
Conflicts of InterestBoth authors hereby declare that there is no conflict of interests whatsoever.
Aportación del estudioEl presente trabajo hace un análisis del efecto en la prescripción que tiene la inclusión de un nuevo medicamento en la guía farmacoterapéutica de un centro hospitalario respecto a todos los fármacos del mismo grupo terapéutico, diferenciando el alcance en 3 niveles asistenciales: hospitalización (pacientes ingresados), consultas externas (pacientes ambulatorios de consultas externas hospitalarias) y servicios de atención primaria de referencia (pacientes ambulatorios atendidos en el centro de salud).
La investigación pretende mostrar como es el viraje y evolución del uso en el conjunto de los Inhibidores de la Bomba de Protones consecuencia de la inclusión del omeprazol en el formulario, y verificar si este comportamiento ayuda o está alineada para conseguir una prescripción más eficiente.
Consideramos es un asunto de sumo interés por su novedad, ya que no hay ningún estudio en España que haya investigado este efecto, por tanto no existe evidencia científica alguna de las consecuencias que tiene la inclusión de un nuevo medicamento en dichas guías en la utilización del resto de fármacos del mismo grupo terapéutico en nuestro país, no sólo en el ámbito de la hospitalización, tampoco en el ámbito de consultas externas (CCEE) del mismo centro, ni en los centros de atención primaria (AP) que tienen como referencia ese mismo hospital donde se ha realizado esta intervención.
IntroducciónLa guía farmacoterapéutica intrahospitalaria, formulario o petitorio de medicamentos, es el listado de aquellos fármacos seleccionados por la Comisión de Farmacia y Terapéutica de ese centro hospitalario disponibles para utilización en pacientes ingresados; es una medida de uso racional en el Sistema Nacional de Salud. Si bien en el ámbito de la atención primaria (AP) algunas áreas han usado este tipo de herramienta, se presenta como recomendaciones, existiendo total libertad para la prescripción fuera de la misma1, a pesar de que algunos países se utilizan en este nivel asistencial con carácter obligatorio2,3.
A la hora de seleccionar los medicamentos a incluir en el formulario lo normal es no considerar el precio que dicho fármaco tiene en la oficina de farmacia4, sin embargo se ha constatado el efecto directo en seguir usando esos medicamentos tras el alta hospitalaria4. En países distintos de España se ha detectado como la prescripción que se realiza a nivel hospitalario tiene una influencia en AP5,6, que parece tener relación directa con los informes de alta y prescripciones en consultas externas7 (CCEE). Otros estudios evalúan la influencia de un cambio en el formulario en las prescripciones extrahospitalarias4, pero ninguno en España.
El gasto farmacéutico en los últimos años en nuestro país ha rondado los 10.000 millones de euros anuales a nivel extrahospitalario8 y en torno a 4.000 millones a nivel intrahospitalario, que pasan a más de 6.000 millones en 2015 si se tiene en cuenta las nuevas terapias farmacológicas contra el virus de la hepatitis C9. Estas cuestiones hacen que en el Servicio de Salud de Galicia (SERGAS), al igual que en otras Comunidades Autónomas, se realice un seguimiento específico de la evolución de la prestación farmacéutica, donde uno de los indicadores utilizados para determinar la eficiencia de prescripción es el Porcentaje de Omeprazol sobre el resto de Inhibidores de la Bomba de protones (IBP) al considerarse éste el IBP de elección por ser el más eficiente. Las áreas sanitarias, o Estructuras Organizativas de Gestión Integrada (EOXI) del SERGAS, son las organizaciones periféricas de dirección ejecutivas que integran la AP y hospitalaria10.
Con la visión de un Servicio de Salud que integra dos niveles asistenciales, parece imprescindible que a la hora de seleccionar un medicamento para ser incluido en el petitorio hospitalario se tenga también en cuenta el precio y el impacto que tendría en la modalidad extrahospitalaria; especial trascendencia tiene este aspecto cuando esta inclusión se considera solo motivada por las bajadas de precio negociadas intracentro, pues podría representar un coste adicional al ser el balance global perjudicial para el conjunto del Servicio de Salud.
En junio de 2014 en el Hospital de Barbanza (Galicia, España) se incluyó en la guía farmacoterapéutica el principio activo omeprazol, estando disponibles en el formulario hasta entonces solamente el pantoprazol y el esomeprazol (éste restringido para pacientes con sonda nasogástrica). En aquel momento en España el coste de una DDD de omeprazol era aproximadamente 10 veces menor que una DDD de cualquier otro IBP 11.
El objetivo de nuestro estudio es analizar el impacto de la introducción de omeprazol en el formulario del hospital de A Barbanza sobre las prescripciones intrahospitalarias (hospitalización) y extrahospitalarias (CCEE y AP) en todo el grupo terapéutico de los inhibidores de la bomba de protones.
MetodologíaEn España está instaurado un aseguramiento sanitario público que abarca prácticamente a toda la población. El presente trabajo de investigación se centra en un hospital de la red del SERGAS; se trata de un hospital comarcal de nivel I12 situado en la localidad de Ribeira en la provincia de A Coruña, con una población adscrita en el año 2014 de 64.287 hab., y de 64.655 en el 201 5, y cuatro servicios de AP de referencia: A Pobra de Cara- miñal (9.186 hab.), Boiro (18.925 hab.), Porto do Son (8.692 hab.) y Ribeira (27.852 hab.). Con 81 camas, la evolución de su índice de ocupación ha sido del 86,16% en el año 2013, 80,80% en el año 2014 y 81,92% en 2015.
Las Dosis Diarias Definidas (DDD) de cada IBP son las unidades básicas de trabajo; nos permiten analizar las secuencias temporales mensuales de consumo de cada principio activo objeto de evaluación. Se define como la dosis media diaria supuesta de un medicamento cuando se usa en su indicación principal. Las DDD, según su la clasificación anatómica de medicamentos13, están en continua revisión por la QMS14. Se establecen las siguientes equivalencias de una DDD: omeprazol (DDD 20 mg), pantoprazol (DDD 40 mg), lansoprazol (DDD 30 mg), rabeprazol (DDD 20 mg) y esomeprazol (DDD 30 mg), tanto para formulaciones orales como parenterales.
Manejar las DDD nos permite realizar estudios comparativos de consumo, independientemente de las variaciones en el precio y en el contenido ponderal de cada presentación comercial. En general, en los estudios descriptivos el número de DDD consumidas en un área o centro se expresa por 1.000 habitantes y por día, denominada Dosis Habitante Día (DHD). Este parámetro nos aproxima al volumen de población tratada diariamente con una dosis habitual de un determinado fármaco, por lo que su uso permite poner de manifiesto diferencias en los hábitos terapéuticos.
En el ámbito ambulatorio el consumo medio se expresa en DHD como se ha dicho, medida que será utilizada para el análisis de CCEE y de AP. Sin embargo, para el cálculo del consumo en hospitales para pacientes ingresados, éste se expresa en forma de DDD por 100 estancias y día15 (DDD/estancias-día) que nos da una estimación de la probabilidad de que un paciente sea tratado con un determinado medicamento durante su estancia hospitalaria, o que es lo mismo, del porcentaje de pacientes hospitalizados tratados con un fármaco determinado durante su estancia. Estas dos unidades, DHD y DDD/estancias-día, son las utilizamos para el cálculo estadístico.
Diferenciamos tres modalidades asistenciales (CCEE, AP y hospitalización) y usamos en todas ellas como medida de eficiencia el porcentaje o proporción de DDD de omeprazol sobre el total de DDD de todos los IBP prescritos, que representamos como: %DDDomeprazol/ DDDtotalIBP.
En cuanto al marco temporal, se realiza un estudio descriptivo retrospectivo durante 36 meses, desde enero de 2013 hasta diciembre de 2015. El cambio en la guía farmacoterapéutica del hospital con la inclusión del principio activo omeprazol se materializa el 6 de junio de 2014, por lo que el presente análisis comprende un periodo similar antes y después de la intervención.
Para obtener los datos de dispensaciones y adquisiciones con cargo al SERGAS se hace una explotación de los sistemas de información corporativos oficiales:
- a.
De todas las dispensaciones realizadas por las farmacias comunitarias del área sanitaria vinculadas a las prescripciones realizadas por facultativos médicos de alguno de los cuatro servicios de AP referencia del hospital y de CCEE del mismo.
La información se obtiene del Sistema de Información de Prestación Farmacéutica en forma de envases dispensados por cada mes, que se transforman en DDD mes y éstos a DHD mensuales.
- b.
De todos los consumos realizados por el servicio de farmacia del hospital de A Barbanza: a través de la explotación de la base de datos del Sistema de Información de Farmacia Hospitalaria que nos ofrece en número de envases consumidos, que se transforma en DDD mes y éstas a DDD/estancias-día.
Para el análisis estadístico construimos un modelo de regresión segmentada de series temporales interrumpido16. La intervención estudiada es la inclusión del principio activo omeprazol en el petitorio del hospital citado.
En este análisis la variable dependiente es DHD o DDD/estancias-día, o los %DDDomeprazol/DDDtotallBP de los distintos IBPs por mes, y las variables independientes son:
- -
El tiempo desde el inicio del estudio que refleja la tendencia temporal previa al cambio en la guía farmacoterapéutica (o intervención).
- -
Una variable binaria que tomó el valor de 0 antes y de 1 después del cambio en la guía, la cual mostraría el cambio inmediato tras la intervención.
- -
Una variable temporal desde el cambio en la guía que tomó el valor de 0 antes de la intervención y después el valor de 1,2,3 que reflejaría el cambio en la tendencia a largo plazo.
El modelo de regresión segmentada realizará 2 rectas de regresión, una con los datos antes del cambio de la guía y otra con los resultados posteriores; proporciona 4 coeficientes (cuando se mencione DHD se podrá extrapolar a DDD/estancias-día o %DDDomeprazol/DDD- totalIBP):
- 1.
Intercepción. Es el punto de corte de la primera recta con el eje Y; representa el valor de DHD estimado por el método de regresión al inicio del estudio. Si el coeficiente no fuese estadísticamente significativo (ES) se podría concluir que el valor de DHD no era distinto de cero al inicio del periodo de estudio.
- 2.
Tendencia previa al cambio en la guía. Es la pendiente de la primera recta; representa el valor de crecimiento o decrecimiento en los valores de DHD antes del cambio. Si el coeficiente no fuese ES se podría concluir que no existía crecimiento o decrecimiento antes del cambio. Si el coeficiente fuese positivo y ES se podría concluir que las DHD estaban creciendo antes de la intervención, y si el coeficiente fuese negativo que las DHD estaban decreciendo antes del cambio.
- 3.
Impacto inmediato del cambio en la guía. Es la diferencia entre el final de la primera recta y el principio de la segunda; representa el salto o bajada inmediata en los valores de DHD. Si el coeficiente no fuese estadísticamente significativo se podría concluir que no ha existido salto o bajada inmediata en los valores. Si el coeficiente fuese positivo y ES se podría concluir que las DHD han sufrido un salto inmediato y si fuese negativo que las DHD han sufrido una bajada inmediata.
- 4.
Cambio en la tendencia tras el cambio en la guía. Es la diferencia entre la pendiente de la segunda recta y la pendiente de la primera, lo cual representa el posible cambio en el crecimiento o decrecimiento a largo plazo en los valores de DHD que se haya podido producir tras la intervención respecto a la velocidad de crecimiento o decrecimiento antes del cambio. Si el coeficiente no fuese ES se podría concluir que no ha existido modificación en el crecimiento o decrecimiento a largo plazo en sus valores respecto. Si el coeficiente fuese positivo y ES se podría concluir que las DHD tras el cambio en la guía han pasado a crecer a mayor velocidad (si antes de la intervención estaban creciendo o estacionarias) o decrecer a menor velocidad (si antes del cambio estaban decreciendo); y si fuese negativo que las DHD han pasado a crecer a menor velocidad (si antes estaban creciendo) o a decrecer a mayor velocidad (si antes estaban decreciendo o estacionarias).
Como medida de ajuste del modelo estadístico usamos el valor de R2.
ResultadosPrimer escenario: Consultas ExternasEn la Figura 1 se muestra la evolución temporal de las DHD de los distintos IBP para prescripciones realizadas mediante receta médica para dispensación extrahospitalaria por médicos del hospital, donde lo más destacado es que las DHD de pantoprazol experimentan un primer descenso brusco para posteriormente pasar a una ligera tendencia creciente.

La regresión segmentada de los datos de DHD de los distintos IBP para CCEE mostró un R2 medio de 0,346. Sus resultados (Tabla 1.a) muestran que el consumo de pantoprazol estaba estacionado antes del cambio en la guía, y tras éste experimenta un brusco descenso ES, para posteriormente pasar a un ligero crecimiento a lar-go plazo también significativo. El consumo de rabeprazol antes del cambio mostraba un crecimiento ES, y tras la intervención no experimenta un cambio inmediato aunque su tendencia posterior a largo plazo resulta un descenso significativo. Para el esomeprazol, que mostraba antes del cambio en la guía una disminución en su utilización significativa, no mostró cambios ES. Los demás IBPs (omeprazol y lansoprazol) no mostraron valores ES, ya sea para la tendencia previa o posterior al cambio en la guía.
Resultados del análisis de la regresión segmentada para los tres escenarios contemplados, enero 2013 a diciembre 2015.
| RESULTADOS DE LA REGRESIÓN SEGMENTADA | a) DHD IBPs para consultas externas | b) DHD IBPs para AP | c) DDD/Estancias-día Hospitalización | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Medicamento | Variable | Coeficiente | IC 95% | P | Coeficiente | IC 95% | P | Coeficiente | IC 95% | P |
| Pantoprazol | Intercepción | 0,618 | 0,520 a 0,716 | <0,001 | 3,774 | 3,315 a 4,233 | <0,001 | 284,648 | 269,064 a 300,232 | <0,001 |
| Tendencia previa al cambio en la guía | 0,004 | -0,006 a 0,014 | 0,445 | 0,066 | -0,010 a 0,142 | 0,102 | 0,283 | -1,238 a 1,804 | 0,718 | |
| Impacto inmediato del cambio en la guía | -0,272 | -0,399 a -0,145 | <0,001 | 0,567 | -0,045 a 1,179 | 0,079 | -32,813 | -53,277 a-12,349 | 0,004 | |
| Cambio en la tendencia tras el cambio en la guía | 0,02 | 0,008 a 0,032 | 0,003 | -0,124 | -0,210 a -0,038 | 0,008 | -4,143 | -6,134 a -2,152 | <0,001 | |
| Omeprazol | Intercepción | 3,006 | 2,443 a 3,568 | <0,001 | 11,278 | 9,845 a 12,711 | <0,001 | 0 | -4,373 a 4,373 | 1 |
| Tendencia previa al cambio en la guía | 0,01 | -0,045 a 0,065 | 0,718 | 0,136 | -0,003 a 0,275 | 0,065 | 0 | -0,427 a 0,427 | 1 | |
| Impacto inmediato del cambio en la guía | 0,05 | -0,734 a 0,744 | 0,99 | 1,003 | -0,879 a 2,885 | 0,304 | 17,249 | 11,506 a 22,992 | <0,001 | |
| Cambio en la tendencia tras el cambio en la guía | 0,05 | -0,068 a 0,078 | 0,887 | -0,075 | -0,257 a 0,107 | 0,43 | 2,856 | 2,297 a 3,415 | <0,001 | |
| Lansoprazol | Intercepción | 0,181 | 0,126 a 0,236 | <0,001 | 3,459 | 3,118 a 3,800 | <0,001 | |||
| Tendencia previa al cambio en la guía | -0,002 | -0,008 a 0,004 | 0,365 | -0,043 | -0,076 a -0,010 | 0,016 | ||||
| Impacto inmediato del cambio en la guía | -0,04 | -0,111 a 0,031 | 0,281 | -0,355 | -0,802 a 0,092 | 0,13 | ||||
| Cambio en la tendencia tras el cambio en la guía | 0,006 | -0,002 a 0,014 | 0,121 | 0,001 | -0,042 a 0,044 | 0,988 | ||||
| Rabeprazol | Intercepción | 0,026 | -0,005 a 0,057 | 0,124 | 1,439 | 1,284 a 1,594 | <0,001 | |||
| Tendencia previa al cambio en la guía | 0,06 | 0,002 a 0,010 | 0,001 | -0,001 | -0,026 a 0,024 | 0,958 | ||||
| Impacto inmediato del cambio en la guía | -0,58 | -0,101 a -0,015 | 0,11 | -0,093 | -0,267 a 0,081 | 0,302 | ||||
| Cambio en la tendencia tras el cambio en la guía | -0,007 | -0,011 a -0,003 | 0,002 | -0,025 | -0,207 a 0,137 | 0,14 | ||||
| Esomeprazol | Intercepción | 0,769 | 0,659 a 0,879 | <0,001 | 2,184 | 1,902 a 2,466 | <0,001 | 1,372 | 0,743 a 2,001 | <0,001 |
| Tendencia previa al cambio en la guía | -0,016 | -0,028 a -0,004 | 0,007 | 0,008 | -0,043 a 0,059 | 0,747 | -0,014 | -0,075 a 0,047 | 0,661 | |
| Impacto inmediato del cambio en la guía | -0,11 | -0,255 a 0,035 | 0,146 | -0,17 | -0,535 a 0,195 | 0,368 | -0,566 | -1,393 a 0,261 | 0,109 | |
| Cambio en la tendencia tras el cambio en la guía | 0,013 | -0,001 a 0,027 | 0,08 | -0,039 | -0,100 a 0,022 | 0,22 | 0,072 | -0,008 a 0,152 | 0,09 | |
Estadísticamente significativo si p<0,05
La Figura 2 muestra la evolución de las DHD de los distintos IBP en los servicios de AP que tienen como referencia el hospital de Barbanza.

La regresión segmentada de los datos de DHD de los distintos IBP para AP mostró un R2 medio de 0,588. Sus resultados (Tabla 1.b)) muestran que las DHD de pantoprazol no experimentaban un crecimiento o decrecimiento antes de la introducción del omeprazol en el petitorio que fuese ES; tampoco se observa un cambio con efecto inmediato ES; no obstante sí se produjo un cambio de tendencia tras la intervención en el sentido de que la utilización de pantoprazol tiende a disminuir a más largo plazo. Las DHD de lansoprazol mostraban una tendencia decreciente antes del cambio en la guía, y tras éste no se percibe ni un salto inmediato ES ni una modificación en la tendencia a largo plazo. Los demás IBP no muestran tendencias ES antes de la intervención, ni saltos o cambios de tendencia posteriores a la misma.
Tercer escenario: HospitalizaciónEn la hospitalización, la Figura 3 muestra que tras el cambio la utilización de pantoprazol a nivel intrahospita- lario pasa a decrecer, la de omeprazol presenta tendencia creciente y la de esomeprazol se mantiene.

La regresión segmentada de los datos de DDD/estancias-día mostró un R2 medio de 0,660. Sus resultados (Tabla 1.c), muestran que el pantoprazol no presentaba crecimiento ni decrecimiento antes del cambio en la guía que fuese ES pero se observa una fuerte disminución inmediata tras la intervención estadísticamente significativa, así como una alteración de la tendencia a largo plazo en el sentido de que la utilización de pantoprazol tiende a decrecer de modo ES. Para el caso del omeprazol se observa de modo ES que tras su inclusión en el petitorio su utilización aumenta inmediatamente, así como su tendencia creciente a largo plazo. Para el esomeprazol no se observa tendencia previa o cambio significativo tras la modificación de la guía.
%DDDomeprazol/DDDtotal IBP en los tres escenariosRespecto al porcentaje de DDD de omeprazol respecto al total de DDD de todos los IBP, la Figura 4 muestra que tras el cambio, a nivel intrahospitalario este porcentaje muestra una clara tendencia creciente, y a nivel de CCEE muestra un salto inmediato para mantenerse estacionario. En este último contexto la evolución de los porcentajes promedio de prescripción de DHD de este principio activo sobre el resto de IBP durante el periodo en estudio es de 72,58%, alcanzando el pico más alto en septiembre de 2014 con un 86,49% (Figura 4). En las prescripciones del ámbito de AP este porcentaje promedio es de 58,14%, en evolución creciente durante todo el estudio.

La regresión segmentada mostró un R2 medio de 0,835. Sus resultados (Tabla 2), muestran que a nivel intrahospitalario se observa que tras la intervención existe un salto inmediato ES y posteriormente una tendencia a largo plazo creciente ES. En CCEE se observa un salto inmediato tras la intervención ES pero la tendencia a largo plazo posterior permanece estacionaria y no es ES. En AP la tendencia a largo plazo antes de la intervención ya era creciente de un modo ES, y no se observa un salto inmediato ES pero sí a largo plazo, en el sentido de que la tendencia de crecimiento se acelera.
Resultados de la regresión para la variable: proporción de DDD de omeprazol sobre el total de IBP.
| Variable | Coeficiente | IC 95% | P | |
|---|---|---|---|---|
| En CCEE hospitalarias | Intercepción | 0,653 | 0,610 a 0,696 | <0,001 |
| Tendencia previa al cambio en la guía | 0,003 | -0,001 a 0,007 | 0,193 | |
| Impacto Inmediato del cambio en la guía | 0,082 | 0,025 a 0,139 | 0,008 | |
| Cambio en la tendencia tras el cambio en la guía | -0,005 | -0,011 a 0,001 | 0,122 | |
| En AP | Intercepción | 0,509 | 0,495 a 0,523 | <0,001 |
| Tendencia previa al cambio en la guía | 0,003 | 0,001 a 0,005 | <0,001 | |
| Impacto Inmediato del cambio en la guía | 0,014 | -0,004 a 0,032 | 0,138 | |
| Cambio en la tendencia tras el cambio en la guía | 0,002 | 0,001 a 0,004 | 0,034 | |
| A nivel ¡ntrahospltalarlo | Intercepción | 0 | -0,012 a 0,012 | 1 |
| Tendencia previa al cambio en la guía | 0 | -0,002 a 0,002 | 1 | |
| Impacto Inmediato del cambio en la guía | 0,058 | 0,042 a 0,074 | <0,001 | |
| Cambio en la tendencia tras el cambio en la guía | 0,011 | 0,009 a 0,013 | <0,001 |
Estadísticamente significativo si p<0,05
En este estudio se observa que existe un claro cambio en la prescripción de los IBP tras la introducción del omeprazol en la guía en las prescripciones intra y extrahospitalarias, especialmente para el pantoprazol. En el primero este cambio es inmediato y marcado, aumentando el porcentaje de omeprazol rápidamente y observándose una tendencia creciente; en CCEE se observa un salto inmediato pero no cambio de tendencia de crecimiento a largo plazo y en AP este porcentaje no presenta un salto inmediato, pero sí un aumento de la velocidad de crecimiento.
En cuanto a la utilización de cada uno de los IBP, a nivel intrahospitalario se observa que tras la introducción de omeprazol en la guía, al mismo tiempo que aumentan DDD/estancias-día de omeprazol, disminuyen las de pantoprazol, mientras que las de esomeprazol permanece estacionaria; esto último ha podido deberse al hecho de que la utilización de esomeprazol ya se encontraba restringida.
A nivel de CCEE no se observa un cambio en las DHD de omeprazol, pero sí una disminución inmediata en las de pantoprazol, así como un cambio de tendencia para las de rabeprazol. El hecho de que se observe cambio en las prescripciones de pantoprazol podría explicarse por los virajes en sus prescripciones intrahospitalarias que finalmente terminan en receta tras el alta; en el caso de rabeprazol al ser su prescripción tan pequeña (DHD media de 0.067) en comparación con los demás IBP (DHD media omeprazol: 3.225) pudo haber provocado que pequeños cambios en la prescripción relativa para los otros IBP tendrían un efecto por desplazamiento muy elevado relativo para él. El que no se observe cambio en las DHD de omeprazol puede ser por su elevado número de DDD previo a la intervención en la guía en CCEE en comparación de las DDD a nivel hospitalario; por ejemplo, si bien en junio de 2014 se usaban 2,947 DHD de omeprazol en CCEE y 18,539 DDD/estancias-día a nivel intrahospitalario, y si tenemos en cuenta que el hospital tiene 81 camas instaladas y 65.000 habitantes, vemos que en junio de 2014 se prescribieron a nivel hospitalario 364 DDD de omeprazol, y en CCEE 5.684 DDD, por lo que la influencia que las primeras puedan ejercer sobre estas últimas es más limitada que la influencia que puedan ejercer las DDD a nivel hospitalario y extrahospitalario de pantoprazol, donde las diferencias no son tan marcadas.
En los médicos de AP tampoco se observa un cambio ES en el omeprazol, pero sí en las prescripciones de pantoprazol en el sentido de que si bien sus DHD no muestran un descenso brusco inmediato, su tendencia a largo plazo pasa a ser decreciente. La explicación podría estar en la prescripción inducida desde CCEE hacia AP17,18,19,21. El que no se observe cambio rápido en las prescripciones de pantoprazol en AP, al contrario que en CCEE, podría deberse a que las DHD de omeprazol en CCEE son muy inferiores a las DHD de omeprazol en AP, en concreto: en CCEE las DHD de omeprazol a junio de 2014 son de 2,947, y su media durante el estudio es de 3,225, frente a la situación en AP donde las DHD a junio 2014 son de 13,647 y su media de DHD durante el estudio de 13,934.
En relación a la evolución de la proporción de DDD de omeprazol respecto a todas las DDD de IBP, el estudio muestra que existe un incremento en todos los niveles, siendo éste inmediato en hospitalización y CCEE, y a más largo plazo en AP. Como el omeprazol es el IBP de elección, la prescripción de IBP pasa a ser más eficiente en los tres escenarios.
No hemos localizado estudios que valoren lo que ocurre en diferentes entornos asistenciales tras la incorporación de un nuevo IBP al formulario de medicamentos intrahospitalario con este enfoque de un análisis longitudinal de series temporales. Sí hemos localizado uno que estudia el impacto del cambio en la guía farmacoterapéutica de un hospital sobre las prescripciones tanto al alta hospitalaria como en un punto varios meses después de la hospitalización4, que evalúa la retirada del esomeprazol por tener un precio 10 veces superior a otro IBP, y lo sustituye por un IBP más eficiente; en este trabajo, que analiza en 3 puntos transversales (antes de la hospitalización, alta y posterior) se encontró que antes del cambio en la guía la mayoría de los pacientes tomaban esomeprazol tanto al alta hospitalaria como meses después, mientras que después de retirarlo la utilización de éste era residual tanto al alta hospitalaria como varios meses después, siendo los IBP eficientes los más usados.
No encontramos trabajos que analicen el efecto de cambio en la guía sobre la prescripción intra y extrahospitalaria a la vez; sí estudios que analizan el efecto extrahospitalario de IBPs tras un cambio en el formulario, y otros que al igual que el nuestro encuentran que el cambio en la guía se asocia a cambios en la utilización del medicamento dentro del hospital22,23.
La prestación farmacéutica debería gestionarse de forma transversal, ya que cambios en las directrices de los centros hospitalarios llevan asociados cambios en los patrones de prescripción. Estos efectos deben ser valorados a la hora de que sean las reducciones de precio determinantes para incluir nuevos medicamentos en las guías farmacoterapéuticas hospitalarias por tener un efecto global24.
Si bien nuestro estudio es ecológico y toda relación de causalidad debe interpretarse con precaución, existen estudios previos que encuentran dicha relación 24. Otra limitación podría ser la no referencia a variables clínicas, sin embargo, en este caso existe evidencia científica suficiente de que ningún IBP presente una eficacia superior al resto en las indicaciones clínicas en las que están aprobados y si se utilizan en dosis equipotentes25, por lo tanto no serian esperadles variaciones de tipo clínico; respecto a la seguridad, tampoco parece haber diferencias en los efectos adversos25.
Por otro lado cabe mencionar que no se ha valorado la evolución de los costes directos de los medicamentos ya que al mes siguiente de realizarse la inclusión del omeprazol entra en vigor una reducción de precios de los IBP26, y una segunda en octubre del año 201 527, importante factor de confusión si se quiere concluir que los cambios en esta variable sean exclusivamente consecuencia de la intervención.
Como conclusión final se puede afirmar que la inclusión en la guía farmacoterapéutica intrahospitalaia del omeprazol ha influido en los patrones de prescripción de los IBP, tanto en hospitalización, como CCEE y en AP, que derivó hacia un uso más eficiente de los mismos.
La inclusión de medicamentos eficientes, o retirada de ineficientes, en el petitorio hospitalario, puede ser una herramienta potencialmente útil y efectiva a largo plazo para mejorar perfiles de prescripción en todos los niveles asistenciales.
Contribuciones de la autoríaRaquel Vázquez Mourelle concibió el presente estudio, y tanto ésta como Eduardo Carracedo Martínez idearon el diseño metodológico del análisis; Raquel Vázquez Mourelle hizo la explotación, validación y transformación de los datos de hospitalización y Eduardo Carracedo Martínez la de CCEEy AP; los dos autores realizaron conjuntamente el análisis y la interpretación de los datos en los tres escenarios que se presentan. La escritura principal del artículo recayó en Raquel Vázquez Mourelle, haciendo Eduardo Carracedo Martínez la revisión crítica de las diferentes versiones con grandes aportaciones intelectuales. Ambos autores aprobaron la versión final del manuscrito.
FinanciaciónNinguna.
AgradecimientosNinguno.
Conflictos de InterésLos dos autores declaran no tener ningún tipo de conflicto de interés.


Farmacia Hospitalaria sigue las recomendaciones para la preparación, presentación y publicación de trabajos académicos en revistas biomédicas
- Inicio
- Todos los contenidos
- Publique su artículo
- Acerca de la revista
- Métricas