


The objective of this study was to reach a consensus on the minimum set of data that would allow to optimize the pharmacotherapy follow-up of patients on biologic agents for chronic systemic inflammatory conditions, through structured and standardized collection with an electronic tool in the hospital pharmacy.
Materials and methodA scientific committee was formed (n = 5 hospital pharmacists). The Delphi Technique was used, 2 rounds of consultation by e-mail for hospital pharmacists. A structured questionnaire was used, based on a bibliographic review and recommendations by the scientific committee; 37 statements were assessed with the Likert 5-point scale (1= „Strongly Disagree“; 5= „Strongly Agree“). Consensus was reached when 75% or more of panel members assigned a score of 1-2 (rejection consensus) or 4-5 (agreement consensus) to the matter reviewed. Descriptive statistical analyses were conducted.
ResultsThe study included 21 hospital pharmacists (70 were invited, there was 70% response). Consensus was reached for 100% of statements. The minimum set of data was agreed upon, as well as the recommendations that the pharmacist had to collect and make during visits: to document the health status, health-related quality of life, changes In treatment compliance and In patient autonomy, as well as the conditions to make feasible the systematic collection of the minimum data set.
ConclusionsThere Is consensus among hospital pharmacists about a minimum data set to be collected, through an electronic tool, which will order, standardize and structure the pharmacotherapy follow-up of patients with chronic Inflammatory conditions on treatment with biologic agents In the Spanish public health system.
El objetivo de este estudio fue consensuar un conjunto mínimo de datos cuya recopilación sistemática y estandarizada, mediante una herramienta electrónica en la farmacia hospitalaria, permitiera optimizar el seguimiento farmacoterapéutico de los pacientes tratados con agentes biológicos por enfermedades sistémicas inflamatorias crónicas. Material y método: Se constituyó un comité científico (n = 5 farmacéuticos hospitalarios). Se empleó la técnica Delphi, 2 rondas de consulta, por correo electrónico entre farmacéuticos hospitalarios. Se utilizó un cuestionario estructurado basado en una revisión bibliográfica y en recomendaciones del comité científico, valorándose 37 afirmaciones en una escala Likert de 5 puntos (1 = „En total desacuerdo“; 5 = „Totalmente de acuerdo“). Se alcanzó consenso cuando el 75% o más de los panelistas puntuaron 1-2 (consenso-rechazo) o 4-5 (consenso-acuerdo) la cuestión planteada. Se realizaron análisis estadísticos descriptivos.
ResultadosParticiparon 21 farmacéuticos hospitalarios (70 invitados, 70% respuesta). Se logró consenso en el 100% de las afirmaciones. Se acordó el conjunto mínimo de datos y de recomendaciones que el farmacéutico debe recoger y hacer en las visitas; documentar el estado de salud, la calidad de vida relacionada con la salud, los cambios en la adherencia al tratamiento y en la autonomía de los pacientes, así como las condiciones para hacer factible la recopilación sistemática del conjunto mínimo de datos.
ConclusionesExiste consenso entre los farmacéuticos hospitalarios en un conjunto mínimo de datos cuya recopilación, mediante una herramienta electrónica, ordenará, estandarizará y sistematizará el seguimiento farmacoterapéutlco de los pacientes con enfermedades Inflamatorias crónicas en tratamiento con agentes biológicos en el entorno sanitario público español.
This study used the Delphi Technique in order to reach consensus between Hospital Pharmacists regarding the minimum set of data, collected in a simple, systematic and standardized way, that would allow to optimize the pharmacotherapy follow-up of patients with chronic systemic inflammatory conditions (rheumatoid arthritis, psoriatic arthritis, ankylosing spondylitis, ulcerative colitis, Crohn's disease and psoriasis) currently receiving biologic agents in Spain.
IntroductionPharmacotherapy follow-up is defined as an intervention aimed at preventing, detecting and solving negative outcomes associated with medication (NOMs) as well as drug-related problems (DRPs)1. It requires involvement and commitment by the Pharmacist, in the outpatient and hospital settings, in terms of being responsible for solving any difficulties reported by patients in this sense, and having a continuous, structured and adequate intervention. This is based upon an active collaboration with patients and the rest of healthcare teams, with the objective of achieving benefits not only at clinical and therapeutical levels, but also in terms of health-related quality of life (HRQoL)1.
The DADER method offers simple guidelines to the Pharmacist in order to conduct a structured pharmacotherapy follow-up, as well as to design a plan of action with the patient, in order to promote intervention continuity over time2. This method has been widely used for setting up pharmacotherapy follow-up, particularly in the outpatient setting, and for chronic patient care3- 4. Some initiatives with similar objectives have been conducted for various conditions, such as hypertension, diabetes mellitus, rheumatoid arthritis, asthma or depression, among others; their purpose is that the Pharmacist can be aware of the essential aspects of health conditions and the medications used for their treatment5-6.
At the same time, there is evidence demonstrating that structuring Pharmacist intervention in chronic patient follow-up is more effective and less costly than the usual non-structured follow-up, even in the setting of geriatric institutions, where one of its benefits is that it leads to a significant reduction in the average number of medicines prescribed to polymedicated elderly patients7.
A systematic collection of data about the medication received by patients seen and followed up at hospital, with a standardization of the different existing pharmacotherapy follow-up methodologies, restructuring the activities included, streamlining the resources available, and prioritizing their basic functions, would lead to a significant improvement in the pharmacotherapy follow-up of patients at hospital8. Additionally, this would be useful in order to promote awareness regarding the clinical role of the Pharmacist in the hospital setting.
Those patients with chronic inflammatory conditions, such as rheumatoid arthritis, psoriatic arthritis, ankylosing spondylitis, ulcerative colitis, Crohn's disease or psoriasis, require thorough attention in terms of the medication received, particularly in the most severe forms of their disease, and when therapeutical regimens become more complex9,10. It is essential to reduce the variability in the use of biologic agents, as well as to watch adherence to biologic treatment, if the objective is to achieve an optimal control of the disease, to recover the functional ability of patients and to improve their HRQoL, while at the same time there is a reduction in the risk-benefit rate of treatment, pharmacological costs are kept low, and equality is ensured in the access to those therapeutic options available11.
The study described here was born out of the need expressed by Hospital Pharmacists about having a minimum set of data, collected in a simple, structured and standardized way, that would allow to optimize the practice of Pharmacists at hospital, as well as the pharmacotherapy follow-up of patients receiving biologic agents for their chronic systemic inflammatory conditions. Given that this standardization requires a wide consensus among the main participants on the adequacy and feasibility of data to be collected, it was suggested to use the Delphi Technique for Consensus, and to explore the opportunity of incorporating said data in an electronic tool specially designed for this aim.
MethodsThe Delphi Technique was used in order to determine the degree of agreement existing between Hospital Pharmacists in terms of the minimum set of information to be considered in the pharmacotherapy follow-up of patients receiving biologic agents for chronic inflammatory systemic conditions; and a series of steps were followed, as shown in Figure 1.

The Delphi Technique consists in an iterative questioning process used for reaching a common point of view regarding different aspects of the stated problem, in order to define potential lines of action12. The rounds of questions were conducted by e-mail, and were designed to meet four essential requirements inherent to the technique13. Firstly, the rounds of questions allowed a repeated and structured confirmation of the opinions by the panel members. E-mail communication allowed to reach participants in distant geographical areas, to facilitate participation because each respondent could answer the questionnaire at the time of day more convenient for them, to keep confidentiality regarding answers, and to reduce the influence of the most dominant individuals over the rest of the group. Finally, the controlled return of answers in the second round reduced the group effect to the minimum, and allowed the statistical aggregation of groups with similar answers.
The Delphi Technique is widely used in the healthcare setting, particularly in studies aimed at exploring the potential scope of implementing policies14, knowledge15, procedures16 and new health technologies17.
Scientific CommitteeA scientific committee was created for the project, formed by five Hospital Pharmacists with experience in the use of biologic agents since their initial introduction in the Spanish Health System. These Pharmacists were expert in the therapeutical management of patients with systemic inflammatory conditions, and were aware of the needs in this group regarding pharmacotherapy follow-up, through the experience transmitted by their team works; they were also promoters of research, education and divulgation in their work centres, and were responsible for decisions around the implementation of new technologies and procedures in their professional settings. One characteristic feature of the scientific committee members was their active participation in academic, political and institutional initiatives in the matter of interest, through scientific societies, and throughout the country.
The scientific committee was in charge of supervising the project development, assessing the adequate use of the information collected in the literature review for preparing the questionnaire to be used in Delphi, defining its characteristics, facilitating the identification of panel members, interpreting its outcomes and encouraging its divulgation.
Literature ReviewWe reviewed the literature regarding the characteristics of pharmacotherapeutic follow-up in patients treated with biological agents as well as the tools designed to systematize and standardize such follow-up. We found 7 publications from which information could be extracted on: the elements that should constitute a tool for pharmacotherapeutic follow-up, main characteristics of a guide for data collection and storage in pharmacotherapeutic follow-up, main opportunities for optimization of follow-up Pharmacotherapeutic and consensuses in the management of inflammatory systemic diseases for its pharmacotherapeutic follow-up. We also identified 7 publications on Health Related Quality of Life, preferences for treatment and satisfaction with the treatment of patients with inflammatory diseases. Finally, the technical files of the biological agents were reviewed with indication in the treatment of the diseases of interest.
Contents of the Delphi Consultation: QuestionnairesBased on the findings of the literature review and the recommendations by the scientific committee, a preliminary version of the first questionnaire to be used in the Delphi Consultation was generated.
This version was assessed by a team of five independent Hospital Pharmacists, selected by the scientific committee, and who would not take part in the subsequent consultation, in order to determine the adequacy of the questions included for the project objective, the clarity of their wording, and the convenience of the scoring scale used. After this test, the first questionnaire included 37 statements classified into two information blocks. The first block referred to the pharmacotherapy follow-up of patients, divided into first visit to the Hospital Pharmacist (14 statements) or subsequent visits (17 statements), and the data to be used to measure the outcomes of pharmacotherapy follow-up (6 statements); the second block explored the scope and utility of an electronic tool implemented to structure the activity by Hospital Pharmacists for patients on biologic treatment for their inflammatory systemic conditions (11 statements). All the questions were written as positive statements, and panel members were asked to assign a score to their level of agreement with them, using a 5-point Likert Scale (1 =Strongly disagree; 5=Strongly agree).
The second round questionnaire included all those questions for which there was no consensus in the first round. The second questionnaire was personalized for each participant; thus, the score assigned by each participant in the first round was stated for each question, as well as the score by the majority of the other participants. Panel members were asked to consider the likelihood of changing their previous score in order to get closer to the position by the majority, or to suggest any changes that they considered relevant for said question.
Selection of panel members for the Delphi ConsultationGiven that the validity of Delphi findings depends mostly of the experience of the persons answering the questions18, the scientific committee of the study recommended a group of Hospital Pharmacists based on selection criteria similar to those described for the scientific committee. Special attention was paid to their affiliation to hospitals of reference in the treatment of moderate and severe systemic inflammatory conditions, with a wide use of biologic agents, and working in Pharmacy Units that were active in the pharmacotherapy follow-up of these patients.
Sample sizeRegarding the number of panel members who should participate in a Delphi Consultation, there is little coincidence among authors about the minimum number of participants19-20. Taking as reference other consensus conducted21-22, it was considered that a minimum number of 20 panel members would be enough for this study, taking into account that they had a thorough knowledge of daily practice.
Invitation and participation of panel membersThe scientific committee members presented a list of persons adequate for being members of the Delphi Expert Panel, and these were contacted and invited to take part in the consultation, after being explained the background and purposes of the study. Once they accepted participating, the first questionnaire of the consultation was sent to them, and they were given two weeks to answer. If there was no response after the third weekly reminder, it was considered that the panel members had turned down their participation. The same procedure was followed in the subsequent round. The first round of consultation was conducted from October, 13th to October, 27th, 2014; and the second round was conducted from November, 17th to November, 30th, 2014. Questionnaires for both rounds were sent and collected as e-mail attachments. The panel members remained anonymous from one another during the entire consultation process.
Definition of ConsensusIt was considered that consensus had been reached when 75% of participants or more gave a 1-2 score, called rejection consensus, or 4-5, called agreement consensus. When 75% of participants or more gave a score of 3, it was considered that the statement was in indeterminacy. If the participants were distributed among the three answer categories, without reaching 75% in any of them, it was considered that consensus had not been reached for said question.
Data AnalysisAfter reviewing that all data had been adequately collected in the questionnaires, the scores given by panel members were included in a Microsoft Excel 2007 database. The frequency and rates of answers were calculated, and the scores given by the set of panel members to each question were described.
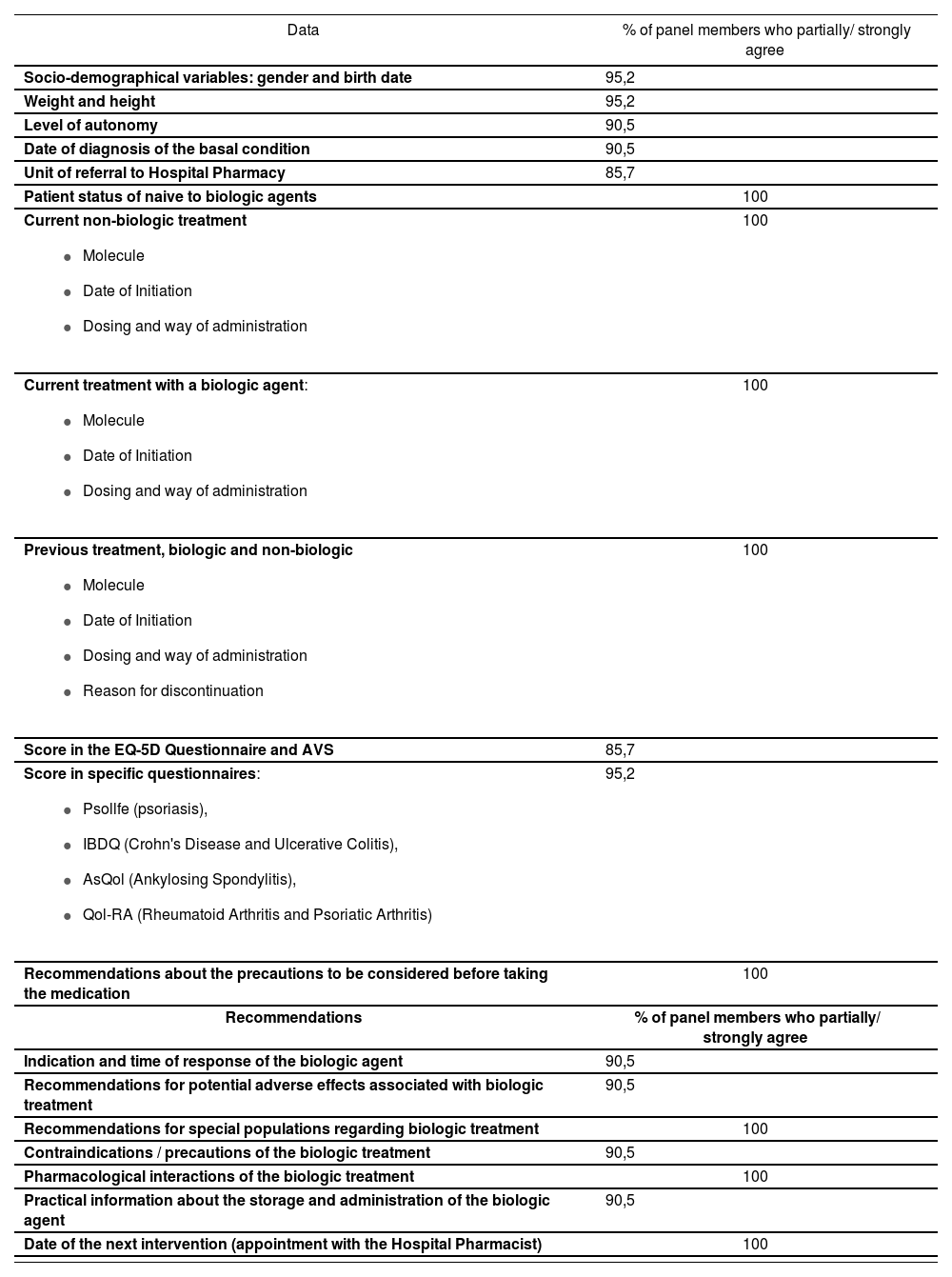
ResultsTwenty-one (21) Hospital Pharmacists participated, out of the 30 initially invited (response rate: 70%), from hospitals in eleven autonomous communities. Between the first and the second consultation rounds, consensus was reached in 100% of the questions stated. It was necessary to clarify two statements, in order to reach an agreement on them in the second round. Tables 1 to 3 show the questions presented, as well as the proportion of panel members with scores between 4 and 5 (partially / strongly agree) at the end of the Delphi Consultation.
Minimum set of recommendations to be made at the first visit
| Data | % of panel members who partially/ strongly agree |
|---|---|
| Socio-demographical variables: gender and birth date | 95,2 |
| Weight and height | 95,2 |
| Level of autonomy | 90,5 |
| Date of diagnosis of the basal condition | 90,5 |
| Unit of referral to Hospital Pharmacy | 85,7 |
| Patient status of naive to biologic agents | 100 |
Current non-biologic treatment
| 100 |
Current treatment with a biologic agent:
| 100 |
Previous treatment, biologic and non-biologic
| 100 |
| Score in the EQ-5D Questionnaire and AVS | 85,7 |
Score in specific questionnaires:
| 95,2 |
| Recommendations about the precautions to be considered before taking the medication | 100 |
| Recommendations | % of panel members who partially/ strongly agree |
| Indication and time of response of the biologic agent | 90,5 |
| Recommendations for potential adverse effects associated with biologic treatment | 90,5 |
| Recommendations for special populations regarding biologic treatment | 100 |
| Contraindications / precautions of the biologic treatment | 90,5 |
| Pharmacological interactions of the biologic treatment | 100 |
| Practical information about the storage and administration of the biologic agent | 90,5 |
| Date of the next intervention (appointment with the Hospital Pharmacist) | 100 |
Measures to assess the outcomes of structuring the pharmacotherapy follow-up
| Measures | % of panel members who partially/ strongly agree |
|---|---|
| Follow-up of dosing prescribed over time (treatment compliance and persistence) | 100 |
| Number of interventions of the Hospital Pharmacist according to the need of referral to physician, or conducted directly on the patient | 100 |
| Number of Hospital Pharmacy interventions per visit | 76,2 |
| Changes in the level of autonomy of the patient that can be explained by the action of treatment with biologic agents | 85,7 |
| Evolution of the score in EQ-5D and AVS | 81 |
Evolution of score in specific questionnaires
| 90,5 |
According to the consensus by panel members, at least the birth date and gender of the patient should be collected during the first visit (socio-demographical variables), as well as a series of anthropometric, clinical and treatment data (Table 1), including weight and height, level of autonomy, date of diagnosis of the basal condition, and referral unit; if it is the first time the patient receives treatment with biologic agents (naïve patient), their current treatment and previous treatments for the condition of interest, both with biologic agents and with other molecules. According to the perception by panel members, enough details should be collected to allow evaluating the therapeutical regimen prescribed (molecule, dates of initiation and ending, dosing regimen and way of administration, reason for discontinuation).
There was agreement about using the EQ-5D questionnaire and AVS to measure the patient-reported perception of their overall health status, as well as using specific questionnaires by condition, such as Psolife (HRQoL Questionnaire for Patients with Psoriasis), IBDQ (Inflammatory Bowel Disease Questionnaire), AsQol (Ankylosing Spondylitis Quality of Life) or Qol-RA (Quality of Life Measure for Rheumatoid Arthritis).
There was consensus about a minimal set of recommendations that Hospital Pharmacists should make during this visit, including an explanation of the indication and the expected time of response with the biologic drug, guidelines for prevention and action against potential adverse effects associated with the current biologic treatment; main contraindications and precautions that should be taken into account when using it, and practical information about medication storage and administration, as well as reminders for subsequent appointment dates (Table 1).
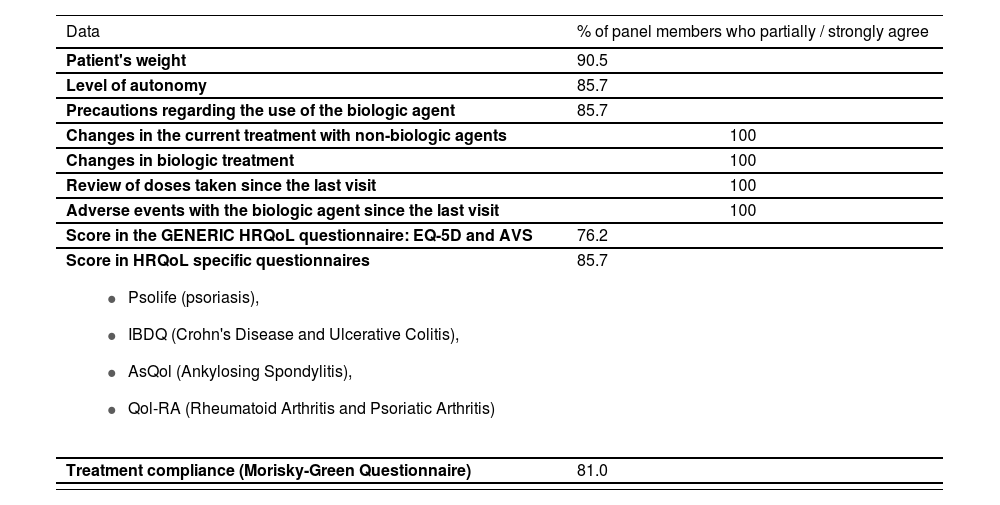
Minimum set of data to be collected in subsequent visits to the Hospital PharmacistThere was agreement that, in subsequent visits and taking the previous visit as reference, patient weight and level of autonomy should be documented, in order to detect any significant changes that required a review of the therapeutic indication; also any modifications prescribed for the treatment with biologic agents and other drugs received by the patient. The adequate compliance of the treatment prescribed should also be verified, by counting the doses since the previous visit; it should be assessed if any adverse effects caused by the biologic agent had appeared since the last visit. The majority of panel members coincided that HRQoL should be measured with the generic EQ-5D questionnaire and its AVS, as well as with specific questionnaires for each condition in subsequent visits, with the purpose of recording their evolution over time; at the same time, it was considered adequate to complete the Morisky-Green Questionnaire to monitor treatment compliance (Table 2).
Minimum set of data to be collected in subsequent visits
| Data | % of panel members who partially / strongly agree |
|---|---|
| Patient's weight | 90.5 |
| Level of autonomy | 85.7 |
| Precautions regarding the use of the biologic agent | 85.7 |
| Changes in the current treatment with non-biologic agents | 100 |
| Changes in biologic treatment | 100 |
| Review of doses taken since the last visit | 100 |
| Adverse events with the biologic agent since the last visit | 100 |
| Score in the GENERIC HRQoL questionnaire: EQ-5D and AVS | 76.2 |
Score in HRQoL specific questionnaires
| 85.7 |
| Treatment compliance (Morisky-Green Questionnaire) | 81.0 |
There was coincidence that, in the second visit, there should be a verification of the precautions required for using biologic agents, while a percentage of participants (4.8%) alerted about the importance of collecting a balanced amount of data, as well as ensuring their record. There has been unanimous agreement about the need to document any interventions by the Pharmacist in all visits.
Frequency of visitsAccording to the suggestions by panel members in the first round, the frequency of visits should depend on whether patients are on treatments with long duration, without changes and controlled disease, or they are naïve patients, or in the initial stage of a new treatment, or with recent changes in treatment. There was consensus, in the second round, that one visit every six months would be adequate for the first scenario and every three months in the latter scenarios (95.2%).
When writing about this aspect, it was clarified that the recommendation about the frequency of patient appointments should be for guidance only, and that professional judgment should prevail over this recommendation.
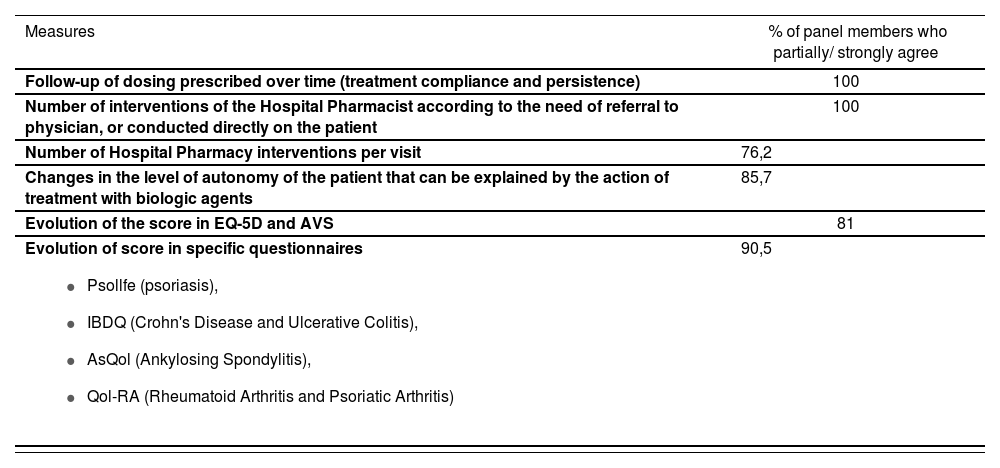
Measures to assess the outcomes of structuring pharmacotherapy follow-upThe adequate treatment follow-up, measured with the Morisky-Green over time, as well as the number of interventions by the Hospital Pharmacist in each visit, either requesting treatment review by the treating physician, providing specific information, or making specific recommendations for an adequate use of biologic agents to the patient, were unanimously acknowledged as feasible measures to demonstrate the optimization of pharmacotherapy follow-up at hospital (Table 3). Consensus was also reached about the importance of documenting the evolution of the autonomy level of the patient, particularly when it can be associated with the use of biologic agents, as well as the scores obtained with EQ-5D and its AVS, and in the specific HRQoL questionnaires, as indicators of a better structured pharmacotherapy follow-up.
Feasibility of collecting the minimum set of data in daily practice at the Hospital PharmacyIn the first round, only 57.1 % of participants agreed partially/strongly with the feasibility of collecting the set of data recommended in daily practice at the Hospital Pharmacy. Various participants highlighted the importance of having an electronic tool integrated into the computer program of the hospital; and that only those changes occurred since the previous visit should be documented in follow-up visits. Including these considerations, 95% of panel members agreed partially or strongly in the second round with the feasibility of the suggested data set collection.
Objectives to be met with the definition of a minimum set of data to be collected at the Hospital PharmacyOne hundred per cent (100%) of participants agreed partially / strongly that the objective of defining a minimum set of data, integrated in an electronic tool into the hospital computer platform, should be the standardization of treatment follow-up for patients with a chronic systemic inflammatory disease on biologic treatment. Reaching an objective of this nature should contribute to the optimization of the healthcare quality provided to this group of patients.
Utility of an electronic tool for pharmacotherapy follow-upIn total, ten questions referred to the utility of an electronic tool that collected this minimum set of data for pharmacotherapy follow-up. One hundred per cent (100%) of participants stated that this would solve unmet needs in Hospital Pharmacy, such as pharmacotherapy follow-up standardization; it would facilitate decision making by the Hospital Pharmacist; it would structure the collection of relevant information consistently and independently from user or patient; it would be useful for an early detection of DRPs and a more effective prevention of the development of NOMs, and it would lead to the creation of a prospective registry of the use of biologic agents in specific conditions, allowing the documentation of any changes, incidences or events associated with treatment, the condition or the patient.
Patient-perceived outcomes of the structured pharmacotherapy follow-upThe majority of participants agreed partially/strongly that a structured and systematic pharmacotherapy follow-up would contribute to improve the adherence of patients to treatment, as well as the perception of their overall health status. This type of interventions would ensure a more personalized follow-up for each patient.
DiscussionThe outcome of this project is the consensus of Hospital Pharmacists regarding a minimum set of data that will allow to order, standardize and structure the pharmacotherapy follow-up of patients on treatment with biologic agents for systemic inflammatory conditions in the Spanish Public Health System. There is agreement about the adequacy of this collection to cover a need still unmet in Hospital Pharmacy practice, and about its feasibility and potential contribution to an optimization of Pharmacy Care for this group of patients. The simplicity of the data set recommended will ensure that these can be easily collected by the different Hospital Pharmacy Units, making it possible to transfer, compare and analyze the results obtained.
Different studies have applied the Delphi Technique in order to define the characteristics of various models for pharmacotherapeutical action targeted to preventing drug-related errors in populations that are particularly vulnerable. This is the case of a 50-expert panel that determined by consensus the set of aspects that should be considered at the time of validating a paediatric medical prescription23. The outcome was a pharmacotherapeutical action model with a series of items grouped into three levels of complexity: basic, intermediate and advanced. The items included in the basic level of the model included sociodemographical variables, such as name, age and gender; anthropometric variables, such as weight and body surface, and other variables associated with the appropriateness of prescription, such as the adequacy of the way of administration, the doses prescribed, and the confirmation of drug interactions, among others. In another publication, a group of 19 experts reached a consensus about the aspects associated with the safety of prescription forms, which should be assessed in order to reduce the incidence of drug-related errors in newborns and paediatric patients24. The methodology used and the results obtained in these studies are very similar to the ones in this study.
There is evidence about the multiple clinical9 and therapeutical8 benefits in patient-perceived health results25; as well as economic benefits7, derived from an adequate pharmacotherapy follow-up.
In this sense, it has been demonstrated that the proactive action by the Hospital Pharmacist will not only contribute to an effective identification and prevention of drug-related problems, both during hospital admission and at discharge and during the subsequent follow-up, but also that their intervention will allow to reduce the time of hospital stay, re-hospitalizations, and the development of secondary conditions26,27.
On the other hand, it is necessary to demonstrate the value added to the healthcare provided by structuring and standardizing patient-follow-up.
The experts understood that the demonstration of the variations in patient attitude towards treatment, which appeared in the answers to the Morisky-Green Questionnaire, as well as the record of the number and nature of the interventions by the Hospital Pharmacist in order to guide, structure or correct treatments with biologic agents, must be used as measures of their intervention outcomes.
Along this line, a group of 26 panel members agreed recently on a set of eight indicators for Hospital Pharmacist action; these included the design of plans for pharmacotherapy follow-up, the provision of education on the condition and the medication, and the promotion of a proactive attitude towards patient treatment follow-up28.
The inclusion of questionnaires, both generic and specific, to measure HRQoL as part of the minimum set of data to be considered for the pharmacotherapy follow-up of patients with inflammatory systemic conditions on treatment with biologic agents, represents a differentiating feature in this consensus. It seems essential to document any changes occurring in this health outcome as an indicator of the adequacy of treatment and pharmacotherapy intervention, given the important compromise of HRQoL in this group of patients, and the significant improvement experienced with the use of biologic treatments29.
An effective pharmacotherapy follow-up will contribute to an improvement in HRQoL, as well as in other patient-perceived results such as treatment compliance and satisfaction, and also in healthcare costs30.
However, the outcomes of this study should be interpreted in the context of its limitations. The Delphi Technique allows to estimate what seems to be more acceptable, acknowledged and feasible, according to the shared opinion by the group of panel members, However, and given that these are agreements regarding healthcare, these outcomes obtained today should be reviewed and updated according to daily practice findings and the dynamic nature of health and its variations over time.
Finally, according to panel members, the inclusion of the minimum set of data in an electronic tool integrated into the hospital computer systems would facilitate their structured collection, as well as their standardization and continuous record over time.
As a conclusion, a minimum set of data has been defined by consensus, which should be collected for a structured and standardized pharmacotherapy follow-up of patients with systemic inflammatory conditions on treatment with biologic agents. This guarantees to facilitate decision making, to structure the collection of relevant data in a consistent manner, to contribute to an early detection of DRPs and a more effective prevention of NOM development, and to allow the creation of a prospective registry of the use of biologic agents for these conditions.
Conflict of interestsBelén Aragón works in MSD; her co-authors received fees for their participation in the project and preparation of the manuscript. However, the authors declare that both the project outcomes and everything described in the manuscript is the result of their free expression, preparation and interpretation of findings.
Aportación a la literatura científicaEste estudio utiliza la técnica Delphi para alcanzar el consenso entre farmacéuticos hospitalarios en la definición de un conjunto mínimo de datos, cuya recopilación sencilla, sistemática y estandarizada permita unificar el seguimiento farmacoterapéutico de los pacientes con enfermedades inflamatorias sistémicas (artritis reumatoide, artritis psoriásica, espondilitis anquilosante, colitis ulcerosa, enfermedad de Crohn y psoriasis) que reciben agentes biológicos en España.
IntroducciónEl seguimiento farmacoterapéutico se entiende como una intervención destinada a prevenir, detectar y resolver tanto resultados negativos de la medicación (RNM) como problemas relacionados con la medicación (PRM)1. Requiere de la implicación y compromiso del farmacéutico, en el ámbito ambulatorio y hospitalario, para responsabilizarse de la resolución de las dificultades que, en este sentido, puedan referir los pacientes, interviniendo de manera continuada, sistematizada y oportuna. Se basa en la colaboración activa con los pacientes y con el resto de los equipos asistenciales con el propósito de alcanzar no sólo beneficios en términos clínicos y terapéuticos, sino también de calidad de vida relacionada con la salud (CVRS)1.
El método DADER ofrece al farmacéutico pautas sencillas para hacer un seguimiento farmacoterapéutico sistematizado así como para diseñar un plan de actuación con el paciente que promueva la continuidad de su intervención en el tiempo2. Este método ha sido ampliamente utilizado en la organización del seguimiento farmacoterapéutico, especialmente en el ámbito ambulatorio y en la atención de los pacientes crónicos3-4. Iniciativas con propósitos similares se han llevado a cabo en diversas patologías como la hipertensión arterial, diabetes mellitus, artritis reumatoide, asma o depresión, entre otros, mediante las cuales se pretende que el farmacéutico conozca los aspectos fundamentales de los problemas de salud y de los medicamentos utilizados para su tratamiento5-6.
A su vez, existe evidencia que demuestra que la sistematización de la intervención del farmacéutico en el seguimiento de los pacientes crónicos es más efectivo y menos costoso que el seguimiento habitual, no sistemático, incluso en el ámbito de las residencias geriátricas donde, entre otros beneficios, contribuye a reducir significativamente el número promedio de medicinas prescritas a los ancianos polimedicados7.
Recopilar sistemáticamente los datos relativos a la medicación que reciben los pacientes atendidos y seguidos en el hospital, unificar las diferentes metodologías de seguimiento farmacoterapéutico coexistentes, reorganizando las actividades que incluyen, optimizando los recursos disponibles y priorizando sus funciones básicas, contribuiría a mejorar sustancialmente el seguimiento farmacoterapéutico de los pacientes en el hospital8. Adicionalmente, serviría para promover la difusión del rol del farmacéutico en las funciones clínicas en el ámbito hospitalario.
Los individuos afectados por enfermedades inflamatorias crónicas como son la artritis reumatoide, artritis psoriásica, espondilitis anquilosante, colitis ulcerosa, enfermedad de Crohn o psoriasis, requieren de una atención minuciosa a la medicación que reciben, especialmente en las formas más severas de la enfermedad y cuando los regímenes terapéuticos son más complejos9-10. Disminuir la variabilidad en el uso de agentes biológicos así como vigilar la adherencia al tratamiento con los mismos es fundamental si el propósito es lograr el control óptimo de la patología, recuperar la capacidad funcional de los pacientes, mejorar su CVRS a la vez que se disminuye la tasa de riesgo-beneficio del tratamiento, se mantienen al mínimo los costes farmacológicos y se procura equidad en el acceso a las alternativas terapéuticas disponibles“.
El estudio que se describe a continuación surge de la necesidad expresada por farmacéuticos hospitalarios de contar con un conjunto mínimo de datos, cuya recopilación sencilla, sistemática y estandarizada permita unificar la práctica farmacéutica en el hospital y el seguimiento farmacoterapéutico de los pacientes que reciben agentes biológicos por enfermedades sistémicas inflamatorias. Dado que su estandarización requiere de un acuerdo amplio entre los principales destinatarios de la idoneidad y factibilidad de los datos a recoger, se propone la técnica Delphi de consenso, y se explora la oportunidad de incorporar dichos datos en una herramienta electrónica especialmente diseñada.
MétodosPara establecer el grado de acuerdo existente entre farmacéuticos de hospital en relación al conjunto mínimo de información que ha de contemplarse en la estandarización del seguimiento farmacoterapéutico de pacientes que reciben agentes biológicos por enfermedades sistémicas inflamatorias crónicas, se utilizó la técnica Delphi y se siguieron una serie de pasos que se muestran en la Figura 1.

La técnica Delphi consiste en un proceso iterativo de consulta que se utiliza cuando se pretende lograr un punto de vista común sobre diversos aspectos de un mismo problema para definir líneas de actuación posibles12. Las rondas de consulta se realizaron por email y fueron diseñadas para cumplir con cuatro requisitos fundamentales e inherentes a la técnica13. Primero, las rondas de consultas sucesivas hicieron posible la comprobación reiterada y sistemática de las opiniones de los panelistas. La comunicación por email permitió llegar a participantes localizados en áreas geográficas distantes, facilitar la participación al poder responder al cuestionario en el momento del día más oportuno para cada participante, mantener la confidencialidad de las respuestas y reducir la influencia de aquellos individuos más dominantes sobre el resto del grupo. Por último, la devolución contro- lada de las respuestas en la segunda ronda minimizó el efecto de grupo y permitió la agregación estadística de grupos con respuestas similares.
La técnica Delphi se emplea ampliamente en el ámbito sanitario, particularmente en estudios que procuran explorar el alcance potencial de implementar políticas14, conocimientos15, procedimientos16 y nuevas tecnologías de la salud17.
Comité científicoSe creó un comité científico para el proyecto constituido por cinco farmacéuticos hospitalarios con experiencia en el empleo de agentes biológicos desde su introducción, por primera vez, en el sistema de salud en España; expertos en el manejo terapéutico de pacientes con enfermedades inflamatorias sistémicas; conocedores de las necesidades en seguimiento farmacoterapéutico de este colectivo por la experiencia transmitida por sus equipos de trabajo; promotores de actividades de investigación, educación y divulgación en sus centros de trabajo, y con responsabilidad de decisión respecto a la implementación de nuevas tecnologías y procedimientos en sus ámbitos de actuación profesional. Un rasgo distintivo de los miembros del comité científico fue su activa participación en iniciativas de carácter académico, político e institucional en el tema de interés a través de las sociedades científicas, y en todo el país.
El comité científico fue el responsable de supervisar el desarrollo del proyecto, de valorar la correcta utilización de la información recopilada en la revisión de la literatura para la elaboración del cuestionario que se utilizaría en el Delphi, de definir sus características, facilitar la identificación de los panelistas, interpretar sus resultados y favorecer su divulgación.
Revisión de la literaturaSe revisó la literatura referida a las características del seguimiento farmacoterapéutico en pacientes tratados con agentes biológicos así como de las herramientas diseñadas para sistematizar y estandarizar dicho seguimiento. Se hallaron 7 publicaciones de las que se ha podido extraer informaciones sobre: los elementos que han de constituir una herramienta de seguimiento farmacoterapéutico, principales características de una guía para la recopilación y almacenamiento de datos en el seguimiento farmacoterapéutico, principales oportunidades para la optimización del seguimiento farmacoterapéutico y consensos en el manejo de enfermedades sistémicas inflamatorias para su seguimiento farmacoterapéutico. Asimismo se identificaron 7 publicaciones sobre Calidad de Vida Relacionada con la Salud, preferencias por el tratamiento y satisfacción con el tratamiento de los pacientes con enfermedades inflamatorias. Finalmente se revisaron las fichas técnicas de los agentes biológicos con indicación en el tratamiento de las enfermedades de interés.
Contenidos de la consulta Delphi: cuestionariosA partir de los hallazgos de la revisión de la literatura y de las recomendaciones del comité científico, se construyó una versión preliminar del primer cuestionario que se utilizaría en la consulta Delphi.
Esta versión fue valorada por un grupo de cinco farmacéuticos hospitalarios independientes, seleccionados por el comité científico y que no participarían en la consulta posterior, para establecer la idoneidad de las cuestiones propuestas para responder al objetivo del proyecto, la claridad en la redacción y la conveniencia de la escala de puntuación propuesta. Tras este testeo, el primer cuestionario quedó compuesto por 37 afirmaciones organizadas en 2 bloques de información, el primero hacía referencia al seguimiento farmacoterapéutico de los pacientes, según se tratase de la primera visita al farmacéutico de hospital (14 afirmaciones) o de visitas sucesivas (17 afirmaciones) y de los datos a utilizar para medir los resultados del seguimiento farmacoterapéutico (6 afirmaciones), el segundo bloque exploraba el alcance y utilidad de una herramienta electrónica implementada para sistematizar la actuación farmacéutica en el hospital en los pacientes con agentes biológicos por enfermedades sistémicas inflamatorias (11 afirmaciones). Todas las cuestiones planteadas se redactaron en sentido positivo (afirmaciones) y se pidió a los panelistas que puntuaran su grado de acuerdo con las mismas en una escala Likert de 5 puntos (1 =En total desacuerdo; 5=Totalmente de acuerdo).
El cuestionario de la segunda ronda incluyó aquellas cuestiones que no alcanzaron consenso en la primera. El segundo cuestionario fue personalizado para cada participante de tal modo que para cada cuestión se indicaba la puntuación otorgada por el mismo participante en la primera ronda, así como la puntuación de la mayoría de los demás participantes. Se pedía a los panelistas que valoraran la posibilidad de cambiar la puntuación previa para acercase a la posición de la mayoría, o bien proponer los cambios que consideraran pertinentes en la cuestión planteada.
Selección de los panelistas para la consulta DelphiDado que la validez de los hallazgos del Delphi, depende fundamentalmente de la experiencia de las personas que responden a la consulta18, el comité científico del estudio propuso a un grupo de farmacéuticos hospitalarios en base a criterios de selección similares a los descritos para el comité científico. Se puso especial atención en que pertenecieran a hospitales de referencia en el tratamiento de enfermedades inflamatorias sistémicas, moderadas y severas, con uso extenso de agentes biológicos, y que operaran en servicios de farmacia activos en el seguimiento farmacoterapéutico de estos pacientes.
Tamaño de la muestraEn relación al número de panelistas que debe participar en un Delphi, existe escasa coincidencia entre los autores sobre la cantidad mínima de participantes19,20. Tomando como referencia otros consensos realizados21,22, en este estudio se consideró que un mínimo de 20 panelistas sería suficiente, teniendo en cuenta su condición de conocedores exhaustivos de la práctica habitual.
Invitación y participación de los panelistasLos miembros del comité científico indicaron una listado de personas idóneas a formar parte del panel de expertos del Delphi, que fueron contactados e invitados a participar en la consulta, tras haberles explicados los antecedentes y propósitos del estudio. Una vez hubieron aceptado participar, se les envió el primer cuestionario de la consulta, y dándoles dos semanas de plazo para responder. Si al cabo del tercer recordatorio semanal no se obtuvo respuesta, se consideró que los panelistas habían declinado su participación. Se procedió de igual modo en la ronda sucesiva. La primera ronda de consulta se realizó entre el 13 y el 27 de octubre de 2014 y la segunda ronda, entre el 17 y el 30 de noviembre de 2014. Los cuestionarios de ambas rondas fueron enviados y recopilados por correo electrónico, como archivo adjunto. Los panelistas permanecieron anónimos, unos a otros, durante todo el proceso de consulta.
Definición de consensoSe consideró que se había alcanzado el consenso cuando el 75% o más de los participantes consultados puntuaron 1-2, denominado consenso rechazo, o 4-5, denominándose consenso acuerdo. Cuando el 75% o más de los participantes puntuaron 3, se consideró que la afirmación estaba en indeterminación. Si los participantes se distribuyeron entre las tres categorías de respuesta, sin alcanzar el 75% en ninguna de ellas, se consideró que no se había alcanzado el consenso en la cuestión propuesta.
Análisis de los datosTras revisar que todos los datos estaban correctamente recogidos en los cuestionarios, las puntuaciones dadas por los panelistas se incluyeron en una base de datos elaborada en Microsoft Excel 2007. Se calcularon las frecuencias y porcentajes de respuesta, describiéndose las puntuaciones otorgadas por el conjunto de los panelistas a cada cuestión planteada.
ResultadosParticiparon 21 farmacéuticos hospitalarios de los 30 inicialmente invitados (tasa de respuesta: 70%) pertenecientes a hospitales de once comunidades autónomas. Entre la primera y la segunda ronda de consulta se alcanzó consenso en el 100% de las cuestiones planteadas. Fue necesario matizar dos afirmaciones para que se lograra el acuerdo en ellas en la segunda ronda. Las cuestiones planteadas así como los porcentajes de panelistas con puntuaciones entre 4 y 5 (parcial/totalmente de acuerdo) al final de la consulta Delphi se resumen en las Tablas 1a3.
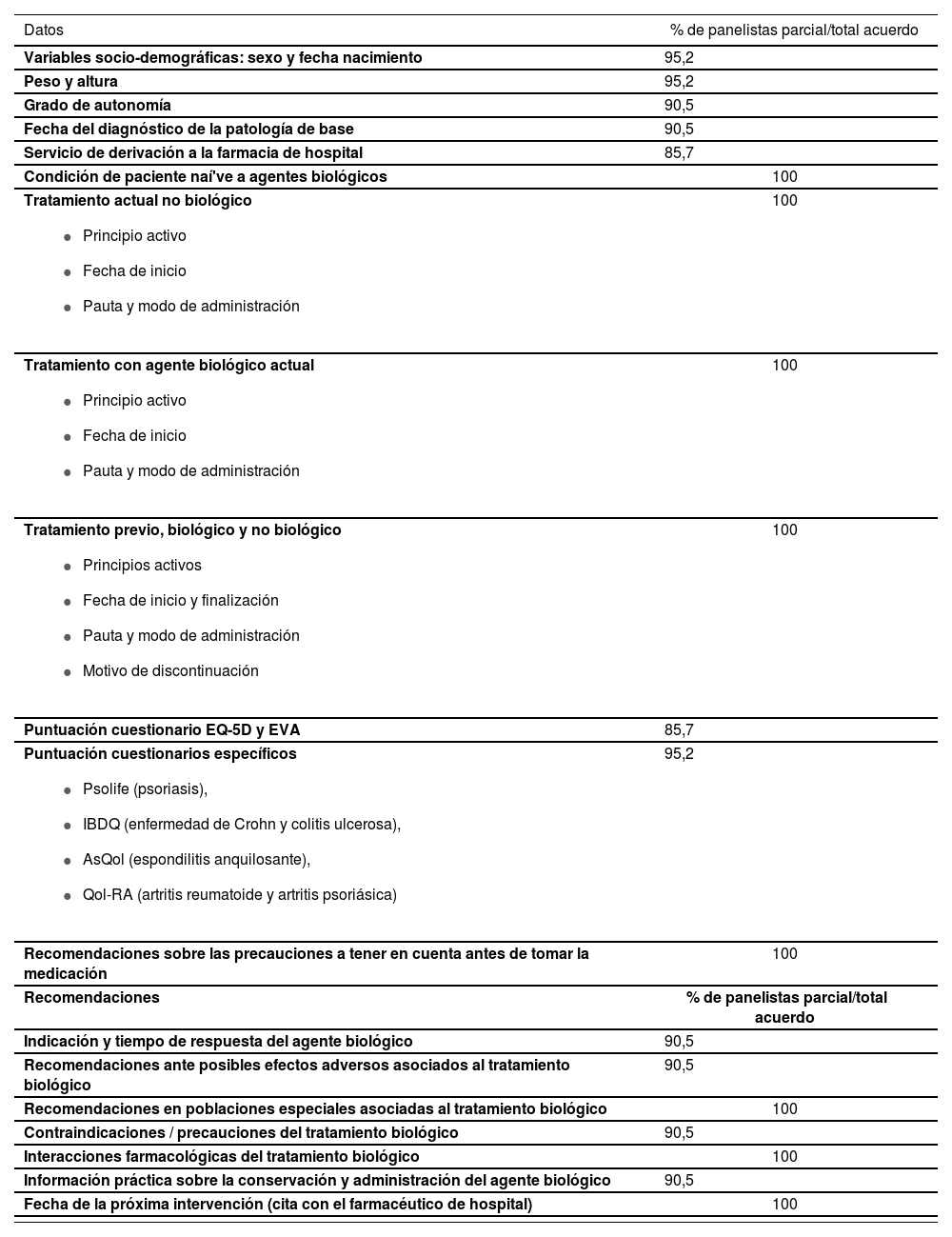
Conjunto mínimo de datos a recoger en la primera visita al farmacéutico del hospitalDe acuerdo con el consenso de los panelistas, en la primera visita han de recogerse, al menos, la fecha de nacimiento y el sexo del paciente (variables socio-demográficas) así como una serie de datos antropométricos, clínicos y de tratamiento (Tabla 1) que incluyen peso y altura, grado de autonomía, fecha del diagnóstico de la patología de base y servicio de derivación; si es la primera vez que recibe tratamiento con agentes biológicos (paciente naïve), su tratamiento actual y los tratamientos previos para la patología de interés, tanto con agentes biológicos como con otros principios activos. De acuerdo con la percepción de los panelistas, debe recogerse el detalle suficiente que permita valorar las pautas terapéuticas indicadas (principio activo, fechas de inicio y finalización, pauta y modo de administración, motivo de discontinuación).
Conjunto mínimo de datos a recoger y recomendaciones a realizar en la primera visita
| Datos | % de panelistas parcial/total acuerdo |
|---|---|
| Variables socio-demográficas: sexo y fecha nacimiento | 95,2 |
| Peso y altura | 95,2 |
| Grado de autonomía | 90,5 |
| Fecha del diagnóstico de la patología de base | 90,5 |
| Servicio de derivación a la farmacia de hospital | 85,7 |
| Condición de paciente naí've a agentes biológicos | 100 |
Tratamiento actual no biológico
| 100 |
Tratamiento con agente biológico actual
| 100 |
Tratamiento previo, biológico y no biológico
| 100 |
| Puntuación cuestionario EQ-5D y EVA | 85,7 |
Puntuación cuestionarios específicos
| 95,2 |
| Recomendaciones sobre las precauciones a tener en cuenta antes de tomar la medicación | 100 |
| Recomendaciones | % de panelistas parcial/total acuerdo |
| Indicación y tiempo de respuesta del agente biológico | 90,5 |
| Recomendaciones ante posibles efectos adversos asociados al tratamiento biológico | 90,5 |
| Recomendaciones en poblaciones especiales asociadas al tratamiento biológico | 100 |
| Contraindicaciones / precauciones del tratamiento biológico | 90,5 |
| Interacciones farmacológicas del tratamiento biológico | 100 |
| Información práctica sobre la conservación y administración del agente biológico | 90,5 |
| Fecha de la próxima intervención (cita con el farmacéutico de hospital) | 100 |
Hubo acuerdo en la utilización del cuestionario EQ-5D y EVA para medir la percepción que refiere el paciente de su estado global de salud y el uso de cuestionarios específicos por patología tales como Psolife (Cuestionario CVRS en el paciente con psoriasis), IBDQ (Inflammatory Bowel Disease Questionnaire), AsQol (Ankylosing Spondylitis Quality of Life) o Qol-RA (Quality of Life Measure for Reumathoid Arthritis).
Hubo consenso en un conjunto mínimo de recomendaciones que debía hacer el farmacéutico de hospital en esta visita, incluyendo una explicación de la indicación y del tiempo de respuesta esperado con el fármaco biológico, pautas preventivas y de actuación ante posibles efectos adversos asociados al tratamiento biológico actual; principales contraindicaciones y precauciones a tener en cuenta con el uso del mismo e información práctica sobre la conservación y administración del medicamento, así como recordar fecha de las próximas citas (Tabla 1).
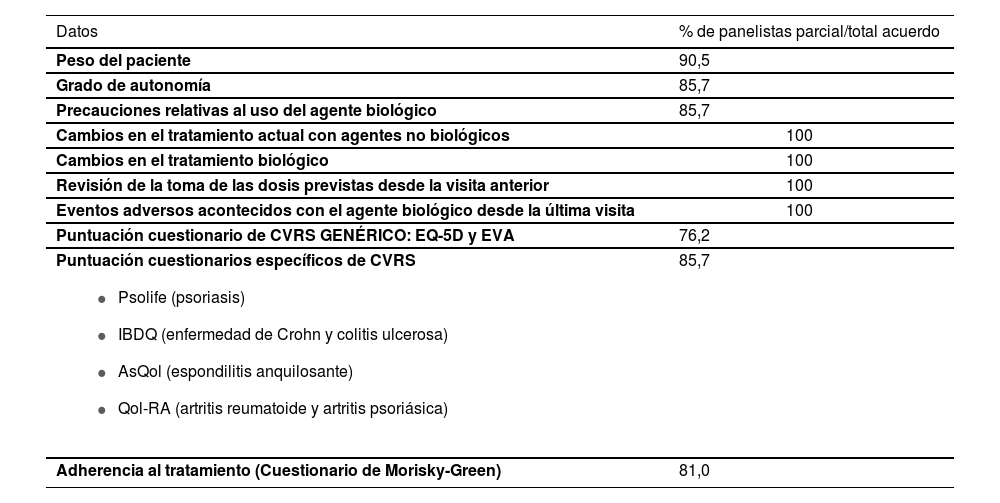
Conjunto mínimo de datos a recoger en las visitas sucesivas al farmacéutico del hospitalExistió acuerdo en que, en visitas posteriores y tomando como referencia la visita previa, se documentaran el peso del paciente y el grado de autonomía para detectar cambios significativos en los mismos que precisen revisar la indicación terapéutica; las modificaciones que se hu-bieran indicado en el tratamiento con agentes biológicos y con otros fármacos que recibe el paciente. Así mismo, verificar el seguimiento correcto de la indicación médica haciendo un recuento de dosis desde la visita anterior; comprobar la existencia, o no, de efectos adversos acontecidos con el agente biológico desde la última visita. La mayoría de los panelistas coincidió en que se midiera la CVRS tanto con el cuestionario genérico EQ-5D y su EVA como con cuestionarios específicos para cada patología en las visitas sucesivas, con el propósito de registrar su evolución en el tiempo del mismo modo que se consideró oportuno cumplimentar el cuestionario de Morisky-Green para monitorizar la adherencia al tratamiento. (Tabla 2)
Conjunto mínimo de datos a recopilar en las visitas sucesivas
| Datos | % de panelistas parcial/total acuerdo |
|---|---|
| Peso del paciente | 90,5 |
| Grado de autonomía | 85,7 |
| Precauciones relativas al uso del agente biológico | 85,7 |
| Cambios en el tratamiento actual con agentes no biológicos | 100 |
| Cambios en el tratamiento biológico | 100 |
| Revisión de la toma de las dosis previstas desde la visita anterior | 100 |
| Eventos adversos acontecidos con el agente biológico desde la última visita | 100 |
| Puntuación cuestionario de CVRS GENÉRICO: EQ-5D y EVA | 76,2 |
Puntuación cuestionarios específicos de CVRS
| 85,7 |
| Adherencia al tratamiento (Cuestionario de Morisky-Green) | 81,0 |
Hubo coincidencia en que, en la segunda visita, se verificaran las precauciones que han de tenerse en el uso de los agentes biológicos mientras que una proporción de participantes (4,8%) alertó sobre la importancia de recopilar una cantidad equilibrada de datos a la vez que se garantiza su registro. En todas las visitas se ha acordado, por unanimidad, la necesidad de documentar las intervenciones realizadas por el farmacéutico.
Frecuencia de visitasDe acuerdo con las sugerencias de los panelistas en la primera ronda, la frecuencia de visitas dependería de si se trata de pacientes con tratamientos de larga dura-ción, sin cambios y enfermedad controlada, o de pacientes nai'ves, o en fases iniciales de un nuevo tratamiento, o con cambios recientes en el mismo. Hubo consenso, en la segunda ronda, en que una visita cada seis meses sería apropiada en el primer supuesto, y cada tres meses en los escenarios últimos (95,2%). En la redacción de este aspecto, se matizó que la recomendación sobre la frecuencia con que debe citarse a un paciente sería orientativa prevaleciendo el criterio profesional sobre esta recomendación.
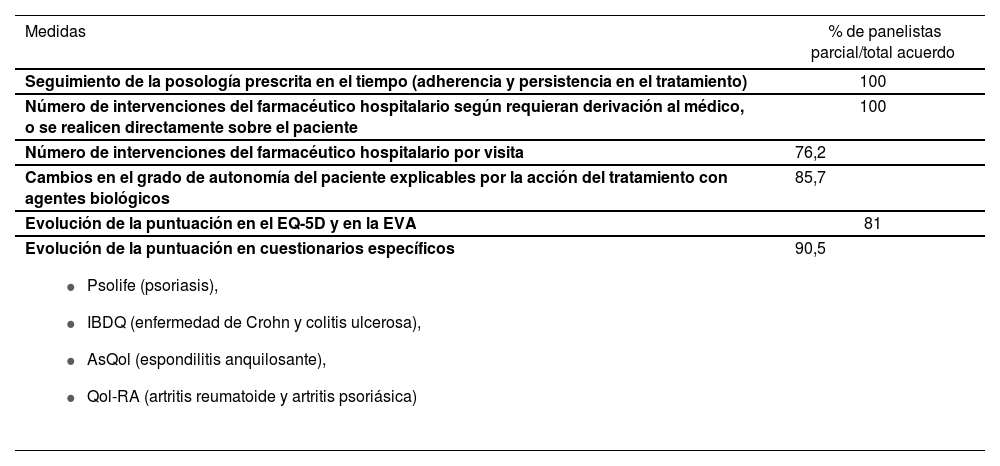
Medidas para valorar los resultados de ordenar el seguimiento farmacoterapéuticoEl correcto seguimiento del tratamiento medido con el cuestionario de Morisky-Green, en el transcurso del
tiempo, así como el número de intervenciones del farmacéutico hospitalario en cada visita, sea solicitando una revisión del tratamiento por el médico responsable, brindando información específica o haciendo recomendaciones concretas para el adecuado uso de los agentes biológicos al paciente, se reconocieron por unanimidad como medidas factibles para demostrar la optimización del seguimiento farmacoterapéutico en el hospital (Tabla 3). Se obtuvo también consenso en la relevancia de documentar la evolución del grado de autonomía del paciente, especialmente cuando pueda relacionarse con el uso de los agentes biológicos, así como de las puntuaciones obtenidas con el EQ-5D y su EVA y en los cuestionarios específicos de CVRS como indicadores de un seguimiento farmacoterapéutico más ordenado.
Medidas para valorar los resultados de ordenar el seguimiento farmacoterapéutico
| Medidas | % de panelistas parcial/total acuerdo |
|---|---|
| Seguimiento de la posología prescrita en el tiempo (adherencia y persistencia en el tratamiento) | 100 |
| Número de intervenciones del farmacéutico hospitalario según requieran derivación al médico, o se realicen directamente sobre el paciente | 100 |
| Número de intervenciones del farmacéutico hospitalario por visita | 76,2 |
| Cambios en el grado de autonomía del paciente explicables por la acción del tratamiento con agentes biológicos | 85,7 |
| Evolución de la puntuación en el EQ-5D y en la EVA | 81 |
Evolución de la puntuación en cuestionarios específicos
| 90,5 |
En la primera ronda, sólo el 57,1 % de los participantes estuvo parcial/totalmente de acuerdo con la factibilidad de recoger el conjunto de datos propuestos en la práctica habitual de la farmacia hospitalaria. Varios participantes destacaron la importancia de contar con una herramienta electrónica que estuviera integrada en el programa informático del hospital y que, en las visitas de seguimiento, sólo se documentaran los cambios que se hubiesen producido desde la visita anterior. Incluyendo estas consideraciones, en la segunda ronda, el 95% de los panelistas estuvo en parcial o total acuerdo con la factibilidad de la recopilación del conjunto de datos sugerido.
Objetivos a cumplirse con la definición de un conjunto mínimo de datos a recopilarse en la farmacia del hospitalEl 100% de participantes estuvo parcial/totalmente de acuerdo con que el objetivo de definir un conjunto mínimo de datos, integrados en una herramienta electrónica en la plataforma informática del hospital debía ser la estandarización del seguimiento del tratamiento con agentes biológicos del paciente con una enfermedad inflamatoria sistémica crónica. Alcanzar un objetivo de esta naturaleza debería contribuir a la optimización de la calidad de la asistencia sanitaria que se brinda a este colectivo de pacientes.
Utilidad de una herramienta electrónica de seguimiento farmacoterapéuticoUn total de diez cuestiones hacían referencia a la utilidad de una herramienta electrónica que recogiera este conjunto mínimo de datos para el seguimiento farmacoterapéutico. El 100% de los participantes indicaron que resolvería necesidades no cubiertas de la farmacia hospitalaria como es la estandarización del seguimiento farmacoterapéutico; facilitaría la toma de decisiones del farmacéutico hospitalario; ordenaría la recopilación de información relevante de manera consistente e independiente del usuario o del paciente; ayudaría a la detección precoz de los PRM; a prevenir más eficazmente la aparición de RNM, y daría lugar a la creación de un registro prospectivo del uso de fármacos biológicos en patologías concretas, permitiendo la documentación de cambios, incidencias o eventos relacionados con el tratamiento, la patología o el paciente.
Resultados percibidos por los pacientes del seguimiento farmacoterapéutico ordenadoLa mayoría de participantes estuvo parcial/totalmente de acuerdo con que el seguimiento farmacoterapéutico, ordenado y sistemático, contribuiría a mejorar la adherencia de los pacientes al tratamiento así como la percepción del estado de salud global. Intervenciones de este tipo harían posible un seguimiento más personalizado de cada individuo enfermo.
DiscusiónEl resultado de este proyecto es el consenso de farmacéuticos hospitalarios respecto a un conjunto mínimo de datos que ha de permitir ordenar, estandarizar y sistematizar el seguimiento farmacoterapéutico de los pacientes en tratamiento con agentes biológicos por enfermedades inflamatorias sistémicas en el entorno sanitario público español. Existe acuerdo en la idoneidad de su recopilación para responder a una necesidad aún no cubierta en la práctica de la farmacia de hospital, en su factibilidad, y en su posible contribución a optimizar la atención farmacéutica en este colectivo de pacientes. La sencillez del conjunto de datos que se proponen garantiza que puedan ser fácilmente recopilados en los diversos servicios de farmacia hospitalaria, haciendo posible la transferencia, comparación y análisis de los resultados obtenidos.
Diversos trabajos han aplicado la técnica Delphi para definir las características de distintos modelos de actuación farmacoterapéutica destinados a prevenir errores asociados a la medicación en poblaciones especialmente susceptibles. Es el caso de un panel de 50 expertos que estableció por consenso el conjunto de aspectos que debían considerarse a la hora de validar una prescripción médica pediátrica23. Como resultado, se obtuvo un modelo de actuación farmacoterapéutica con una serie de ítems agrupados en tres niveles de complejidad: básico, intermedio y avanzado. Los ítems incluidos en el nivel básico del modelo comprendían variables sociodemo- gráficas, como nombre, edad y sexo; antropométricas como peso y superficie corporal, y otras relativas a la adecuación de la prescripción, como son la idoneidad de la vía de administración, las dosis indicadas, y la comprobación de interacciones medicamentosas, entre otras. En otra publicación, un grupo de 19 expertos consensuaron los aspectos relativos a la seguridad de los formularios de prescripción que debían valorarse para reducir la incidencia de errores asociados a la medicación en neonatos y pacientes pediátricos24. Tanto la metodología utilizada como los resultados obtenidos en estos trabajos son muy similares a los de este estudio.
Existe evidencia de los múltiples beneficios clínicos9, terapéuticos8, en resultados en salud percibidos por los pacientes25 y económicos7, derivados de un adecuado seguimiento farmacoterapéutico.
En este sentido, se ha demostrado que la actuación proactiva del farmacéutico de hospital no solo contribuye a identificar y prevenir efectivamente problemas relacionados con la medicación, tanto durante el ingreso en el hospital como al alta y durante el seguimiento posterior, sino que su intervención permite reducir el tiempo de estancia en el hospital, los reingresos y la aparición de enfermedades secundarias26-27.
Por otra parte, es necesario demostrar el valor añadido que aporta la sistematización y estandarización del seguimiento de los pacientes a los cuidados sanitarios que se les brindan.
Los expertos entendieron que la demostración de las variaciones que se produjeran en la actitud del paciente frente al tratamiento y que se reflejaran en las visitas sucesivas, así como el registro del número y naturaleza de las intervenciones que el farmacéutico hospitalario hiciera para orientar, organizar o subsanar los tratamientos con agentes biológicos han de servir como medidas de resultado de su intervención.
En esta línea, recientemente, un grupo de 26 panelistas acordaron un set de ocho indicadores de resultado de la actuación del farmacéutico de hospital entre los que se incluían el diseño de planes para el seguimiento farmacoterapéutico, la provisión de educación sobre la patología y la medicación, y la promoción de una actitud proactiva con el seguimiento del tratamiento en el paciente28.
La inclusión de cuestionarios, tanto genéricos como específicos, para medir la CVRS como parte del conjunto mínimo de datos que ha de contemplarse en el seguimiento farmacoterapéutico de pacientes con enfermedades sistémicas inflamatorias en tratamiento con agentes biológicos podría considerarse un rasgo distintivo de este consenso. Parece fundamental documentar los cambios que se producen en este resultado en salud como un indicador de la adecuación del tratamiento así como de la intervención farmacoterapéutica dado el importante compromiso de la CVRS en este colectivo de pacientes y la mejora significativa que experimentan con el uso de agentes biológicos29.
El seguimiento farmacoterapéutico efectivo no solo contribuye a mejorar la CVRS, sino también otros resultados percibidos por los pacientes como son la adherencia al tratamiento y la satisfacción así como los costes de los cuidados sanitarios30.
Sin embargo, los resultados de este estudio deben interpretarse en el contexto de sus limitaciones. La técnica Delphi permite estimar aquello que, en opinión compartida por el grupo de panelistas, parece más aceptable, reconocido y factible. No obstante, y tratándose de acuerdos relativos a los cuidados sanitarios, los resultados hoy obtenidos deberán revisarse y actualizarse en función de los hallazgos de la práctica habitual y del carácter dinámico y variable en el tiempo del fenómeno de la salud.
Finalmente, de acuerdo con los panelistas, la inclusión del conjunto mínimo de datos en una herramienta electrónica integrada en los sistemas informáticos de los hospitales facilitaría la sistematización de la recopilación de los mismos, su estandarización y el registro continuado a lo largo del tiempo.
En conclusión, se ha definido un conjunto mínimo consensuado de datos a recoger para el seguimiento farmacoterapéutico sistematizado y estandarizado de pacientes con enfermedades inflamatorias sistémicas en tratamiento con agentes biológicos que promete facilitar la toma de decisiones, ordenar la recopilación de información relevante de manera consistente, ayudar a la detección precoz de los PRM y a prevenir más eficazmente la aparición de RNM, y permitir la creación de un registro prospectivo del uso de agentes biológicos en estas patologías.
AgradecimientosLos autores agradecen muy sinceramente la participación de los siguientes profesionales y sus equipos de trabajo como panelistas en el Delphi: Amparo Burgos San José (Hospital General Universitario de Alicante), Carlos Codina Jané (Hospital Clínic), Luis Carlos Fernández Lison (Hospital de Cáceres), Cristina García Yubero (Hospital Infanta Sofía), Ma Ángeles González Fernández (Hopital La Paz), Ana Iglesias Lambarri (Hopital de Galdako), Alberto Jiménez Morales (Hospital Universitaro Virgen de las Nieves), Palmira Jolonch Santasusagna (Hospital Lleuger Santa Tecla), Alicia Lázaro López (Hospital Universitario de Guadalajara), Amparo Lluch Colomer (Hopital Universitario Virgen del Rocío), Julio Martínez Cutillas (Hospital Valí d'Hebron), Alicia Martínez Hernández (Hospital Infanta Sofía), Emilio Molina Cuadrado (Hospital Torre- cárdenas), Emilio Monte Boquet (Hospital Universitari i Politécnic La Fe), Oihana Mora Atorrasagasti (Hospital de Galdako), Andrés Navarro Ruiz (Hospital General de Elche), Juan José Ortiz de Urbina-Glez (Hospital Virgen Blanca), Marisol Rodríguez Cobos (Hospital Universitario de Santiago (CHUS), Amelia de la Rubia Nieto (Hospital Universitario Virgen de la Arrixaca), Ramón Sanmiguel Elcano (Hospital de Navarra), Ma José Vázquez Castillo (Hospital Universitario de Móstoles). También agradecen la colaboración del equipo de Outcomes'10 por su colaboración en el desarrollo del proyecto y en la redacción de este manuscrito.
FinanciaciónEste proyecto ha sido financiado por Merck Sharp & Dohme (MSD)
Conflicto de interesesBelén Aragón trabaja en MSD; los co-autores recibieron honorarios por su participación en el proyecto así como por la elaboración del manuscrito. No obstante, los autores declaran que tanto los resultados del proyec- to como lo descrito en el manuscrito responde a su libre expresión, elaboración e interpretación de los hallazgos.


Farmacia Hospitalaria sigue las recomendaciones para la preparación, presentación y publicación de trabajos académicos en revistas biomédicas
- Inicio
- Todos los contenidos
- Publique su artículo
- Acerca de la revista
- Métricas