
The last few years have seen an increase in the use of opioid analgesics and in the incidence of opioid overdoses. The objective of this study was to evaluate the number of overdose-related visits to a university hospital emergency department at two different periods of time to analyze potential differences in terms of patient characteristics, prescription profile, and treatment.
MethodThis is a retrospective observational study of opioid overdose-related visits in two periods of time: 2009-2014 and 2018-2020.
ResultsThe study included 47 cases of opioid overdoses: 20 during the first period (3.3 cases/year) and 27 during the second (9 cases/year). A comparison between the two period showed a decrease in the patients’ age (81.1 vs 74.0; p = 0.044) and an increase in the number of acute trauma-derived pain treatments at the expense of chronic pain treatments (p = 0.002). No differences were observed in the opioids involved. As regards symptoms, there was a decrease in the incidence of confusional syndromes (p = 0.026) and an increase in deaths.
ConclusionsEmergency room visits for opioid overdoses have increased in recent years, as has the mortality associated to them. A change has also been observed in the profile of affected patients, with a higher number of cases where pain is derived from acute trauma.
El uso de fármacos opioides ha aumentado en las últimas décadas, así como las intoxicaciones relacionadas con su uso. El objetivo de este estudio es evaluar el número de visitas a urgencias en un hospital universitario por intoxicaciones por opiáceos entre dos periodos y analizar las posibles diferencias de las características de los pacientes, perfil de prescripción y el tratamiento de dicha intoxicación.
MétodoEstudio observacional, retrospectivo de las visitas debidas a intoxicaciones por fármacos opiáceos en dos periodos: 2009-2014 y 2018-2020.
ResultadosSSe incluyeron 47 casos de intoxicaciones, 20 en el primer periodo (3,3 casos/año) y 27 en el segundo (9 casos/año). Se observó una disminución en la edad de los pacientes (81,1 versus 74,0; p = 0,044) y un incremento de tratamientos debidos a dolor traumatológico agudo a expensas de menos tratamientos de dolor crónico (p = 0,002). No hubo diferencias en el opiáceo implicado. Con respecto a la clínica, se observó una disminución en los síndromes confusionales (p = 0,026) y un incremento de fallecimientos.
ConclusionesLas visitas a urgencias por intoxicaciones a fármacos opiáceos han aumentado en los últimos años, así como la mortalidad asociada. El perfil de los pacientes implicados ha variado, incrementándose el tratamiento de dolor traumatológico agudo.
Given their effectiveness in the treatment of pain, opioids have become a widely used analgesic that was prescribed to over 11 million patients in the US in 20161. Yet, one in five deaths in Americans aged 24 to 34 years has been attributed to opioid overdoses2, which has become a true epidemic. Although use of opioids in Spain has also become more widespread in the last decade3, the data available on inappropriate use and its consequences remains scarce4.
The last few years have seen an increase in the number of emergency room visits prompted by opioid intoxication events. The purpose of this study was therefore to carry out a comparative analysis of intoxicationrelated emergency room visits by patients on active opioid treatment in two different periods of time. Another goal was to analyze possible outcome differences related to patients’ characteristics, prescription profiles, and the treatment indicated for the intoxication. The study was carried out in a third-level university hospital.
MethodsThis was a retrospective observational study of all the opioid overdose-related visits to the emergency room of a third-level hospital. All adult patients diagnosed with an intoxication following active ambulatory treatment with opioids between 2018 and 2020 (t1) were included in the study. The data obtained was compared with that of a historical series extending from 2009 to 2014 (t2). Improper and/or recreational opioid users were excluded from the study.
The hospital's toxicology unit has a database with information on all medication-induced intoxications that must be treated at the emergency room. Cases were identified by means of a review of diagnoses given at discharge from the hospital's emergency room containing the terms intoxication, overdose, ingestion, and opioid. The idea was to identify those cases where the reason for presentation at the emergency room was an intoxication caused by a prescribed opioid analgesic. Data was extracted from the patients’ electronic medical records (EMRs). The information collected included demographic data (age, sex), medical history, prescribing department, opioid involved, indication for the prescription, symptoms of the intoxication, complications, administered treatment and where the patient was transferred on discharge. The contribution of intoxication to the patients’ death was classified based on clinical criteria and the EXITOX mortality register into unquestionable, very likely or likely5.
The statistical study was performed with the SPSS v25.0 for Windows software package. Values were expressed as means (standard deviation) or percentages. Student's t test was used for comparisons of means, while the chi-squared test with Fisher's Exact Test correction was used for comparisons of proportions, if required. Statistical significance was assumed if p < 0.05.
The study was approved by the hospital's Research Ethics Committee.
ResultsForty-seven emergency room visits prompted by opioid overdoses were included in the study. Twenty of them occurred during t1 (3.3 cases/year) and 27 during t2 (9 cases/year). The percentage of opioid overdoses with respect to all toxic substance/medicine-induced intoxications treated during t1 was 0.48% (of a total of 4,141) and rose to 1.38% (of a total of 1,961) in t2 (p < 0.001).
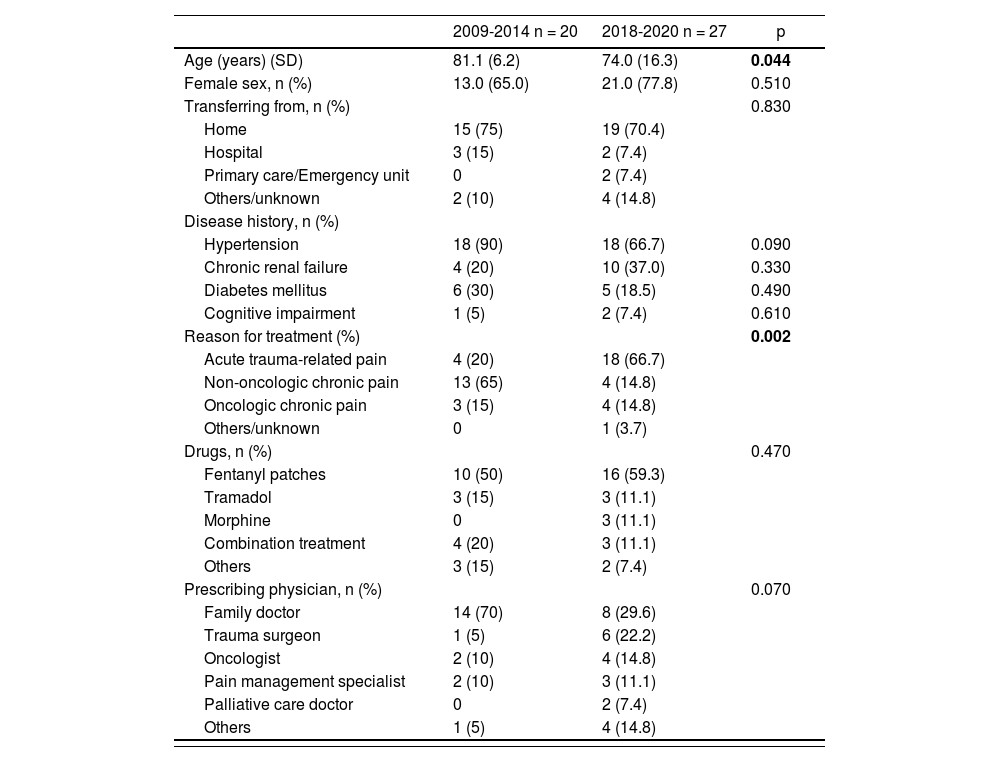
Table 1 shows the patients’ characteristics. The population in the two periods was rather heterogeneous as regards age and indication for treatment. Mean age was significantly lower in t2 [81.1 (6.2) vs 74.0 (16.3) years; p = 0.044]. The majority of patients in the two periods were women, most of whom had been transferred to the emergency room from their homes. No significant differences were found with respect to disease history. The reason for prescribing opioids was predominantly related to the presence of non-oncological chronic pain in t1 and trauma-related pain in t2 (p = 0.002), with fentanyl patches being the most commonly used medication in both periods (50.0% and 59.3%). Although family doctors were the most common prescribers, prescriptions by these healthcare providers shrank considerably in t2 (70.0% vs 29.6%) as compared with those made by trauma surgeons (5.0% vs 22.2%); this difference was however not statistically significant.
Characteristics of patient suffering from opioid-induced intoxication
| 2009-2014 n = 20 | 2018-2020 n = 27 | p | |
|---|---|---|---|
| Age (years) (SD) | 81.1 (6.2) | 74.0 (16.3) | 0.044 |
| Female sex, n (%) | 13.0 (65.0) | 21.0 (77.8) | 0.510 |
| Transferring from, n (%) | 0.830 | ||
| Home | 15 (75) | 19 (70.4) | |
| Hospital | 3 (15) | 2 (7.4) | |
| Primary care/Emergency unit | 0 | 2 (7.4) | |
| Others/unknown | 2 (10) | 4 (14.8) | |
| Disease history, n (%) | |||
| Hypertension | 18 (90) | 18 (66.7) | 0.090 |
| Chronic renal failure | 4 (20) | 10 (37.0) | 0.330 |
| Diabetes mellitus | 6 (30) | 5 (18.5) | 0.490 |
| Cognitive impairment | 1 (5) | 2 (7.4) | 0.610 |
| Reason for treatment (%) | 0.002 | ||
| Acute trauma-related pain | 4 (20) | 18 (66.7) | |
| Non-oncologic chronic pain | 13 (65) | 4 (14.8) | |
| Oncologic chronic pain | 3 (15) | 4 (14.8) | |
| Others/unknown | 0 | 1 (3.7) | |
| Drugs, n (%) | 0.470 | ||
| Fentanyl patches | 10 (50) | 16 (59.3) | |
| Tramadol | 3 (15) | 3 (11.1) | |
| Morphine | 0 | 3 (11.1) | |
| Combination treatment | 4 (20) | 3 (11.1) | |
| Others | 3 (15) | 2 (7.4) | |
| Prescribing physician, n (%) | 0.070 | ||
| Family doctor | 14 (70) | 8 (29.6) | |
| Trauma surgeon | 1 (5) | 6 (22.2) | |
| Oncologist | 2 (10) | 4 (14.8) | |
| Pain management specialist | 2 (10) | 3 (11.1) | |
| Palliative care doctor | 0 | 2 (7.4) | |
| Others | 1 (5) | 4 (14.8) |
SD: standard deviation.
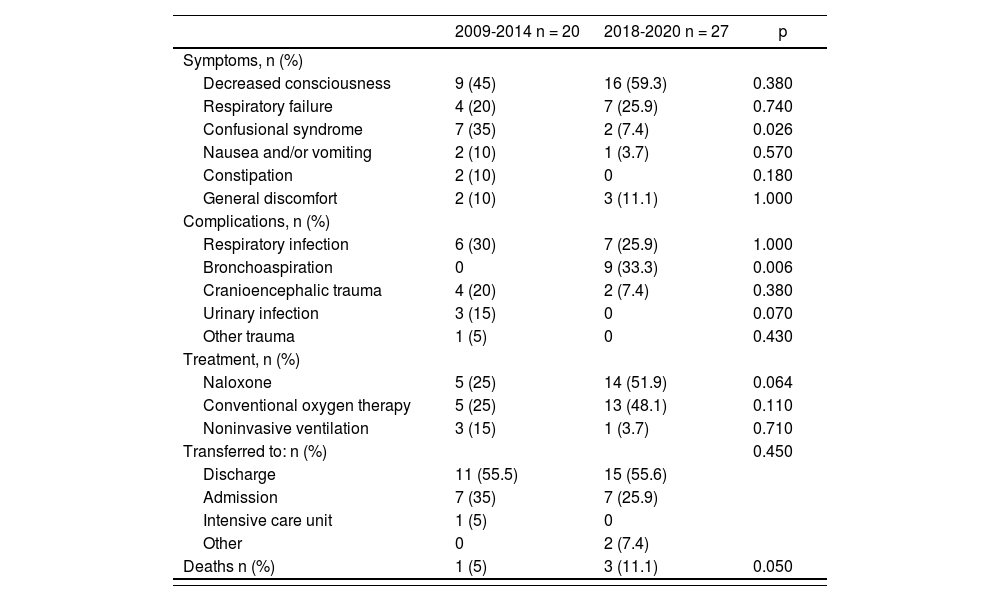
The characteristics of the intoxication episodes are shown in table 2. No differences were found regarding the patients’ symptoms, except with respect to the incidence of confusional syndrome, which was lower in t2 (35.0% vs 7.4%; p = 0.026). As far as complications are concerned, there were 9 cases of bronchoaspiration (33.3%), all of them in t2 (p = 0.006). A trend was observed toward a more assiduous use of naloxone in t2 (25.0% vs 51.9%; p = 0.064). One death occurred in t1 and three in t2.
Characteristics of the intoxication episode
| 2009-2014 n = 20 | 2018-2020 n = 27 | p | |
|---|---|---|---|
| Symptoms, n (%) | |||
| Decreased consciousness | 9 (45) | 16 (59.3) | 0.380 |
| Respiratory failure | 4 (20) | 7 (25.9) | 0.740 |
| Confusional syndrome | 7 (35) | 2 (7.4) | 0.026 |
| Nausea and/or vomiting | 2 (10) | 1 (3.7) | 0.570 |
| Constipation | 2 (10) | 0 | 0.180 |
| General discomfort | 2 (10) | 3 (11.1) | 1.000 |
| Complications, n (%) | |||
| Respiratory infection | 6 (30) | 7 (25.9) | 1.000 |
| Bronchoaspiration | 0 | 9 (33.3) | 0.006 |
| Cranioencephalic trauma | 4 (20) | 2 (7.4) | 0.380 |
| Urinary infection | 3 (15) | 0 | 0.070 |
| Other trauma | 1 (5) | 0 | 0.430 |
| Treatment, n (%) | |||
| Naloxone | 5 (25) | 14 (51.9) | 0.064 |
| Conventional oxygen therapy | 5 (25) | 13 (48.1) | 0.110 |
| Noninvasive ventilation | 3 (15) | 1 (3.7) | 0.710 |
| Transferred to: n (%) | 0.450 | ||
| Discharge | 11 (55.5) | 15 (55.6) | |
| Admission | 7 (35) | 7 (25.9) | |
| Intensive care unit | 1 (5) | 0 | |
| Other | 0 | 2 (7.4) | |
| Deaths n (%) | 1 (5) | 3 (11.1) | 0.050 |
Fentanyl patches were the medication involved in two of the patients who died; oxycodone was involved in one case and codeine in another. Indications for treatment were non-oncologic chronic pain in three patients and oncologic pain in the other. Treatment with opioid analgesics was considered to contribute to death in all cases, and to be likely to be the decisive contributing factor in two cases (a patient receiving palliative treatment with oxycodone for pain control, and a patient where the fentanyl dose was upped to control non-oncologic pain).
DiscussionThe results of this study show that opioid analgesic-induced intoxications have become more common in the last few years. The number of intoxications recorded in t2, which only included the last three years, was higher than in t1, which underscores the need to develop intoxication prevention strategies. Moreover, a few changes were observed in the characteristics of the affected patients between the two periods, such that in t2 patients were younger and most had acute trauma-related conditions. This also led to a change in the prescriber's profile, with trauma surgeons being the main prescribers during t2. Although the complexity of the intoxications and their resulting complications did not in general experience too many changes between the two periods, it must be noted that the number of deaths increased threefold. However, the deaths occurred in patients treated for chronic pain, without there being any connection between those deaths and the higher number of opioid-induced intoxications among patients with trauma-related conditions, who were the ones where the greatest increase in prescriptions was observed.
The age of patients visiting the emergency room in connection with opioid overdoses decreased in t2 from 81 to 74 years. Despite this increase in mean patient age, this finding confirms the data previously reported by our group indicating that opioid-induced intoxications occur mostly in patients over 65 years of age6, although the most commonly affected age group is that of patients between 76 and 85 years7. The predominance of patients older than 65 years was confirmed by a subsequent multicenter study8. The mean age reduction observed in this study could be due to the increased prescription of opioids for treating non-oncologic acute (particularly trauma-related) pain, which tends to occur in younger patients. This increase in the number of patients with acute pain treated with opioid analgesics is in line with the findings of a Chilean study, which reported that up to 7% of patients discharged from the emergency room were prescribed treatment with these drugs, particularly for non-oncologic acute pain9.
The absence of bronchoaspiration during t1 must be taken cautiously. Due to the retrospective nature of this study, it cannot be ruled out that some of the complications classified as respiratory infections during t1 were not in fact bronchoaspirations. The diagnoses considered were those reflected in the patients’ discharge reports. Decreased levels of consciousness tend to predispose subjects to bronchoaspiration, which means that the difference between a diagnosis of bronchoaspiration and one of respiratory infection is, at best, debatable.
Although the overall complexity of the episodes leading to emergency room visits did not change too much between t1 and t2, there was a trend toward an increase in the number of deaths which, though small in absolute terms, should lead to an increased awareness of the importance of keeping these patients under close surveillance. Even if all the deaths analyzed in this study occurred in patients with chronic pain, strict strategies should be developed to monitor and prevent inappropriate use of opioid analgesics at the beginning of treatment and to optimize their administration as a function of the patients’ clinical situation, any physiopathological changes in their metabolism, and the drug's clearance rate. Optimization of the changes of active ingredients is also essential. The above mentioned Chilean study found that prescriptions were in many cases lacking in information, which could induce patients to make mistakes while taking the medication8. For these reasons, the health authorities of the United States have issued as series of precise recommendations related to the indications and dosing of, and time of treatment with, opioid analgesics in order to limit potential adverse events and deaths related with their use10-12. Such recommendations should also be introduced in Spain13.
The limitations of this study include its retrospective nature as well as its small sample size. Nonetheless, the increase in the number of cases observed between the two periods, albeit not as alarming as that observed in other countries, does point to the importance of closely monitoring this problem.
FundingNo funding.
Conflict of interestNo conflict of interests.
Contribution to the scientific literature
This study describes the characteristics of the opioid-derived intoxications observed in the last decade.
Analyzing the profile of intoxications resulting in visits to the emergency room could help design strategies to follow-up and prevent inappropriate use of opioid analgesics.
Early Access date (07/04/2021).

