



The primary endpoint is to validate the HIV Symptoms Index Questionnaire in a Spanish population, in terms of comprehension and acceptability. The secondary endpoints are to describe symptoms reported by patients, tolerance, and quality of life.
MethodThe pilot trial of an observational and multicenter non-comparative study, for the validation of the HIV Symptoms Index Questionnaire in a Spanish population. Patients over the age of 18 diagnosed with HIV infection and receiving treatment were included. The symptoms index, treatment adherence based on pharmacy dispensing records, and quality of life with MOS-HIV questionnaire were calculated. Statistical analyses were conducted with the SAP System V9.2.
ResultsBetween 2013 and 2014, the HIV Symptoms Index Questionnaire was applied to 75 patients; 95% of these patients considered the questionnaire was easy to apply and understand. The total median score of the questionnaire was nine symptoms (IQR 1-18); and the most frequent symptoms were nerves or anxiety (45%), stomach swelling, pain or gas (40%), sleep problems (39%), and fatigue or lack of energy (37%). Presence of symptoms was associated with a worse outcome in the MOS-HIV questionnaire. According to the Visual Analogue Scale, the higher the score in the questionnaire, the lower the tolerance level (R = –0.51; p < 0.0001), and the higher number of days with symptoms (R = 0.51; p < 0.0001).
ConclusionsThe questionnaire was easy to apply. A high tolerance level was confirmed, as well as a consistent and significant correlation with the MOS-HIV and the Visual Analogue Scale.
El objetivo principal es validar el cuestionario de Indice de Síntomas de VIH en población española, en cuanto a comprensión y aceptabilidad. Objetivos secundarios: describir síntomas referidos por el paciente, tolerancia y calidad de vida.
MétodoFase piloto de un estudio observacional y multicéntrico no comparativo, para la validación del cuestionario de Indice de Síntomas de VIH en población española. Se incluyeron pacientes mayores de 18 años, diagnosticados de infección por el VIH en tratamiento. Se calculó el índice de síntomas, la adherencia según los registros de dispensación y la calidad de vida con el cuestionario MOS-HIV. Los cálculos estadísticos se realizaron en el SAP System V9.2.
ResultadosSe aplicó el cuestionario de Indice de Síntomas de VIH en 75 pacientes, durante los años 2013 y 2014. El 95% consideró el cuestionario como de fácil aplicación y comprensión. La mediana de la puntuación total del cuestionario fue de nueve síntomas (RIQ 1-18); y los síntomas más frecuentes fueron: nervios o ansiedad (45%), hinchazón, dolor o gas en el estómago (40%), dificultad para dormir (39%) y cansancio o falta de energía (37%). La presencia de síntomas se relacionó con un peor resultado en el cuestionario MOS-HIV. Según la escala visual analógica, cuanto mayor era la puntuación en el cuestionario, menor era el nivel de tolerancia (R = –0,51; p< 0,0001) y mayor el número de días con síntomas (R = 0,51; p < 0,0001).
ConclusionesLa aplicación del cuestionario fue sencilla. Se constata un nivel de tolerancia alto; y una correlación consistente y significativa con el MOS-HIV, así como con la escala visual analógica.
High-activity antiretroviral treatment (ART) has contributed greatly to control the human immunodeficiency virus (HIV) infection, significantly reducing its morbimortality1. This requires high adherence to the treatment prescribed. The presence of adverse effects, both at short and long term, has become a determining factor, and clearly associated with lack of treatment adherence, mainly because these are strongly associated with the patient's quality of life2–7.
The best way to assess adverse effects in the patient is to conduct direct interviews; this is known as Patient Reported Outcomes. The questionnaire prepared by Justice et al., “HIV Symptom Index”8, is the only questionnaire validated for the determination and follow-up of symptoms reported by patients on ART, and its use is supported by the American AIDS Clinical Trials Group (ACTG), which refers to it as “Symptoms distress module”8.
Due to the lack of questionnaires validated for the Spanish population in order to measure symptoms perceived by the patient with HIV infection, this research team intends to validate the HIV Symptoms Index (HSI) by Justice; the goal is that its application in daily clinical practice can be helpful to improve the detection and management of treatment-related adverse effects 9.
The HSI Questionnaire consists of 20 questions about specific HIV symptoms, and takes into account symptoms reported by patients as well as their intensity.
The primary objective of the study is to evaluate the HSI Questionnaire in terms of its comprehension, acceptability and clarity. As secondary objective, it intends to describe symptoms reported by the patient and their level of tolerance, as well as their quality of life.
MethodsThe pilot trial of an observational and multicenter non-comparative study was conducted; it was called “Tolerometer”, and used for the validation of the 20-question HSI Questionnaire by the ACTG, with an additional question to indicate any other symptom not collected, and two more to assess the level of overall tolerance and the number of days with poor tolerance, through a Visual Analogue Scale (VAS).
The study included patients over the age of 18, diagnosed with HIV infection and on ART treatment (at least for one month), who granted their Informed Consent in writing, were attending personally the Pharmacy Outpatient Units, and were able to understand and answer the questionnaires.
The criterion widely accepted in literature and suggested by Conelly for the pilot study was used for calculating the sample size: it should be at least 10% of the sample estimated for fieldwork. It was calculated that for the subsequent study, at least 115 patients would be needed for questionnaire validation10.
Patients were recruited prospective and consecutively from July, 2013 to February, 2014, in 5 hospitals. After recruitment, information was collected both directly from the patients and from their clinical record.
Initially, a pre-test was conducted in order to evaluate the comprehension of the original questionnaire; this pre-test was answered by 17 patients from the Primary Researcher center. Subsequently, they underwent a cognitive interview, in order to evaluate question comprehension and their relevance according to the opinion of the persons who answered them.
Sociodemographical variables were collected: gender, age, level of studies, occupational status; also disease-related variables: time since diagnosis, group of risk, CDC classification, presence of Hepatitis C, CD4 level and viral load. Variables associated with their current ART were also collected: Naive vs. previously treated, time on ART, current treatment (drugs, dose, number of tablets and frequency of administration), duration of their current treatment, other concomitant treatments (particularly treatment for hepatitis C).
A descriptive analysis was conducted on the sample analyzed, estimating means and standard deviations (medians and interquartile ranges in case normal distribution was not followed) for continuous variables, as well as frequencies and percentages for categorical variables.
The HIV Symptoms Index was calculated by adding up the result of each of the 20 questions, with values ranging between 0, if lack of symptom, and 4, if symptom very bothersome. A total value between 0 and 80 could be reached. A symptom was considered “bothersome” when it was valued as “It bothers me” or “It bothers me a lot”. An extra question was added to the HSI questionnaire, in order to collect any symptom not shown; it also included two analogue scales to detect the level of tolerance and the frequency.
The questionnaire takes into account those symptoms occurred within the four previous weeks.
Patients also answered a qualitative opinion questionnaire in order to understand the time of application and the difficulty and level of comprehension of the questionnaire, as well as any suggestions for improvement.
Based on the hypothesis that the quality of life of the patient will be worse with a higher number of symptoms, the specific MOS-HIV quality of life questionnaire was applied. Said questionnaire is one of the most widely used in order to evaluate health-related quality of life in HIV infection; it has even been used as gold standard to develop and validate other questionnaires11.
The MOS-HIV questionnaire consists of 35 questions on 11 health dimensions, with an overall score ranging from 0 to 100, where a higher score indicates a better health status. Additionally, two indexes are obtained, one for mental health and another for physical health. It refers to the last two weeks, it is easy to apply and can be self-administered. It has demonstrated validity, reliability and sensitivity to change12. Besides, it has been translated and validated for the Spanish population, where it has been widely used.
The association of the scores obtained was evaluated with the presence / lack of symptoms for each item of the questionnaire of specific symptoms, according to the level of symptomatology reported by each physical and mental component of the MOS-HIV. For this aim, Wilcoxon non-parametric test was applied for independent samples. Pearson's correlation index was calculated, in order to evaluate the association between the values in each item and the total index of specific symptoms with the level of tolerance and the frequency of the VAS.
Adherence was estimated through the Medication Possession Ratio (MPR), obtained from the Pharmacy Dispensing Records during at least three months before applying the questionnaire, and preferably in a six month interval. Besides, the SMAQ (Simplified Medication Adherence Questionnaire) was applied, since is validated in the Spanish HIV population, which measures treatment adherence during the four previous weeks, the same period as the HSI13.
Statistical analysis were conducted with the SAS System V9.2 statistical package; statistical significance was assumed when p < 0.05.
This study was conducted according to the principles by the Declaration of Helsinki; it was also authorized by the Ethics Committee for Clinical
Research from the Basque Country, and classified as a post-authorization observational study of prospective follow-up.
ResultsIn the Pilot phase, the HSI questionnaire was applied to 75 patients in the Pharmacy Units of all five hospitals. The mean age of the population was 43.5 (SD 12.1) years, and they were mostly male (73%), as shown in Table 1.
Descriptive analysis of sociodemographic and clinical variables
| Variables | N (%) |
|---|---|
| Total | 75 |
| Gender | |
| – Male | 55 (73.33) |
| – Female | 20 (26.67) |
| Age | 43.48 (12.06)* |
| Level of studies | |
| – No studies | 8 (10.66) |
| – Primary school | 26 (34.67) |
| – Secondary school | 20 (26.67) |
| – Tertiary Education | 2 (2.67) |
| – University | 18 (24.00) |
| – NA | 1 (1.33) |
| Occupational status | |
| – Unemployed | 28 (37.33) |
| – Employed by others | 32 (42.67) |
| – Freelance worker | 6 (8.00) |
| – Retired | 9 (12.00) |
| Route of infection | |
| – Homosexual | 19 (25.33) |
| – Heterosexual | 23 (30.67) |
| – PDUs | 26 (34.67) |
| – NA | 7 (9.33) |
| CDC Classification | |
| – A | 31 (41.33) |
| – B | 3 (4.00) |
| – C | 12 (16.00) |
| – NA | 29 (38.67) |
| HCV Co-infection | |
| – No | 56 (74.67) |
| – Yes | 16 (21.33) |
| – SVR | 3 (4.00) |
| No. of lymphocytes CD4 cell/μL | 648.59 (316.66)* |
| Undetectable viral load | 64 (85.33) |
| Number of treatments | |
| – Naive patients | 14 (18.67) |
| – Previously treated | 58 (77.33) |
| – NA | 3 (4.00) |
| PIlls per day | 2,81 (1.74)* |
| MPR adherence | 94,41 (7.66)* |
| No. of days for adherence | 194,95 (70.55)* |
| Frequency of administration | |
| – BID | 11 (14.67) |
| – QD | 62 (82.67) |
| – ND | 2 (2.66) |
| Concomitant HCV treatment | 2 (2.67) |
| Other concomitant treatments | 28 (37.33) |
Regarding clinical data, 85% of patients presented undetectable viral load, and the CD4 lymphocytes mean level was 648.6 cell/µL (SD 316.7); 19% of naive patients, with a mean number of pills per day of 2.8 (SD 1.7), most of them administered once a day (83%). Of these patients, 37% had other concomitant treatments besides ART, and 2.7% were on treatment for Hepatitis C.
The majority were receiving treatment based on two Nucleoside Reverse Transcriptase Inhibitors (NRTIs) plus 1 Non-Nucleoside (NNRTI) (37); 19 patients in combination with a boosted Protease Inhibitor (bPI), and two in combination with an Integrase Inhibitor (INI). Of the remaining 17 patients, eight were receiving a bPI as monotherapy, four as dual therapy based on bPI, and five with at least three drugs of different classes.
The median overall score of the HSI was 9 (IQR 1-18) on a scale from 0 to 80. No symptom was reported by 19% of patients, while 57% of patients experienced no bothersome symptoms. At the same time, the median number of symptoms reported by patient was 5 (IQR 1-10); and the median number of bothersome symptoms reported by patient was 0 (IQR 0-3).
The most frequent symptom detected in the HSI questionnaire was nerves or anxiety (45%), followed by stomach swelling, pain or gas (40%), sleep problems (39%) and tiredness or lack of energy (37%). When only bothersome symptoms were considered, the most frequent were anxiety and stomach swelling (20%) and sleep problems (17%). Table 2 shows every symptom with its reporting frequency.
Descriptive analyses of the HSI Questionnaire
| Description of symptom | N (%) | |
|---|---|---|
| Frequency of symptoms | Frequency of bothersome symptoms | |
| 1. Tiredness/lack of energy | 28 (37.33) | 8 (10.67) |
| 2. Fever, shivering, sweating | 13 (17.33) | 4 (5.33) |
| 3. Vertigo or dizziness | 19 (25.33) | 2 (2.67) |
| 4. Pain, numbness, itching | 15 (20.55) | 4 (5.48) |
| 5. Difficulty remembering | 26 (34.67) | 10 (13.33) |
| 6. Nausea or vomiting | 20 (27.03) | 6 (8.11) |
| 7. Diarrhoea or loose stools | 26 (34.67) | 6 (8.00) |
| 8. Feeling of sadness or depression | 26 (35.14) | 7 (9.46) |
| 9. Nerves or anxiety | 34 (45.33) | 15 (20.00) |
| 10. Sleep disorders | 29 (38.67) | 13 (17.33) |
| 11. Skin problems | 21 (28.00) | 6 (8.00) |
| 12. Coughing or breathing problems | 13 (17.57) | 2 (2.70) |
| 13. Headache | 22 (29.33) | 7 (9.33) |
| 14. Loss of appetite/change in taste | 19 (25.33) | 4 (5.33) |
| 15. Stomach swelling, pain or gas | 30 (40.00) | 15 (20.00) |
| 16. Pain in muscles or joints | 23 (31.08) | 10 (13.51) |
| 17. Problems in sexual relationships | 26 (34.67) | 8 (10.67) |
| 18. Changes in body appearance | 27 (36.00) | 10 (13.33) |
| 19. Weight loss problems | 17 (22.67) | 4 (5.33) |
| 20. Hair loss or changes | 18 (24.00) | 6 (8.00) |
| Total HSI Score [0-80]* | 9 [1-18] | |
| Level of Tolerance AVS* | 9 [8-10] | |
| Frequency of Tolerance AVS* | 0 [0-2] | |
There were four patients reporting symptoms not collected in the original questionnaire, with their level of discomfort: arthritis-osteoarthritis (very bothersome), intense dreams (slightly bothersome), irritability (slightly bothersome), and heat and sweating (not bothersome).
According to the results of the qualitative opinion questionnaire, the mean time needed to complete the questionnaire was 11 minutes (range from 1 to 33 minutes); 58 patients (77%) completed it on their own. Most patients considered the questionnaire was simple and easy to understand (94.7%), while three patients found it difficult; 89% of patients considered that the questionnaire was useful.
Only three patients answered that they could not associate some questions with their treatment, while there were some very similar questions; they did not report any specific symptom stated that was not well understood, and no suggestion was made in order to improve the questions.
Four patients said that some matter or important symptom was missing, such as gastric discomfort and hot flushes.
Suggestions offered by 12 patients were collected; five of them found the questionnaire was long and included repeat questions, though some patient considered it too brief. Someone suggested repeating the questionnaire periodically, and someone else pointed out the option of taking note even of little things.
The median tolerance level according to the VAS was 9 (IQR 8-10), and the number of days with poor tolerance was 0 (IQR 0-2).
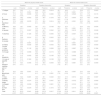
The median Level of Tolerance VAS was 10 (IQR 9-10) in the group of patients with lack of symptoms vs. 9 (IQR 7-10) among those patients reporting some symptom; this difference was significant (p = 0.008). This piece of data was repeated in the Frequency of Tolerance VAS (p = 0.02), as appears in Table 3.
Association between tolerance and frequency with the AVS and specific symptoms
| Level of Tolerance AVS | Frequency of Tolerance AVS | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ISV | Symptom | Symptom discomfort | Symptom | Symptom discomfort | ||||||||
| Lack | Presence | p-value | Lack | Presence | p-value | Lack | Presence | p-value | Lack | Presence | p-value | |
| 1. Fatigue | 9 [9-10] | 8 [7-9.5] | 0.0076 | 9 [8-10] | 6.5 [5.3-7.5] | 0.0027 | 0 [0-1] | 1.5 [0-3] | 0.0009 | 0 [0-1] | 2.5 [2.53] | 0.0003 |
| 2. Fever | 9 [8-10] | 8 [5-9] | 0.0223 | 9 [8-10] | 5 [4.5-5.5] | 0.0014 | 0 [0-1] | 1 [0-3] | 0.1677 | 0 [0-1] | 2.5 [1.5-4] | 0.0088 |
| 3. Dizziness | 9 [8-10] | 8 [5-10] | 0.0160 | 9 [8-10] | 5 [4-6] | 0.0294 | 0 [0-1] | 1 [0-3] | 0.0212 | 0 [0-1] | 1.5 [1-2] | 0.1860 |
| 4. Hand/Foot Pain | 9 [8-10] | 8 [5-9] | 0.0047 | 9 [8-10] | 4.5 [3.5-6.5] | 0.0032 | 0 [0-1] | 1 [0-5] | 0.0018 | 0 [0-1] | 6.5 [3-9] | 0.0017 |
| 5. Memory Loss | 9 [9-10] | 8 [7-10] | 0.0123 | 9 [8-10] | 8 [5-10] | 0.2197 | 0 [0-1] | 1 [0-3] | 0.0217 | 0 [0-1] | 0.5 [0-3] | 0.3869 |
| 6. Nausea | 9.5 [8-10] | 7.5 [6-9] | 0.0014 | 9 [8-10] | 5.5 [5-7] | 0.0074 | 0 [0-1] | 1.5 [0-2.5] | 0.0103 | 0 [0-1] | 2.5 [2-5] | 0.0036 |
| 7. Diarrhea | 10 [9-10] | 8 [6-9] | 0.0006 | 9 [8-10] | 7 [5-9] | 0.0609 | 0 [0-1] | 1.5 [0-3] | 0.0035 | 0 [0-1] | 5 [2-8] | 0.0011 |
| 8. Sadness | 9 [9-10] | 8 [7-10] | 0.0287 | 9 [8-10] | 6 [5-10] | 0.2510 | 0 [0-1] | 1.5 [0-4] | 0.0016 | 0 [0-1] | 2 [0-5.5] | 0.0912 |
| 9. Anxiety | 9 [9-10] | 8 [6-10] | 0.0029 | 9 [8-10] | 8 [5-10] | 0.1588 | 0 [0-1] | 1 [0-3] | 0.0059 | 0 [0-1] | 0 [0-5] | 0.2300 |
| 10. Sleep Trouble | 9 [8-10] | 8 [7-10] | 0.1560 | 9 [8-10] | 8 [5.5-10] | 0.3539 | 0 [0-1] | 1 [0-3] | 0.0011 | 0 [0-1] | 1 [0-3] | 0.1058 |
| 11. Skin problems | 9 [8-10] | 9 [6-10] | 0.0991 | 9 [8-10] | 7 [4-10] | 0.2066 | 0 [0-1] | 0 [0-3] | 0.1813 | 0 [0-1] | 0.5 [0-5] | 0.4005 |
| 12. Cough | 9 [8-10] | 9 [7-10] | 0.8125 | 9 [8-10] | 7.5 [5-10] | 0.7279 | 0 [0-2] | 0 [0-1] | 0.9425 | 0 [0-1.5] | 2.5 [0-5] | 0.5102 |
| 13. Headache | 9 [8-10] | 8 [7-10] | 0.0659 | 9 [8-10] | 8 [6-10] | 0.1836 | 0 [0-1] | 1 [0-3] | 0.0114 | 0 [0-1] | 2 [0-5] | 0.0280 |
| 14. Loss of appetite | 9 [8-10] | 9 [6-10] | 0.2945 | 9 [8-10] | 7 [4.5-9.5] | 0.2427 | 0 [0-1] | 0 [0-2] | 0.7720 | 0 [0.1] | 1.5 [0.5-3.5] | 0.1492 |
| 15. Stomach swelling, pain or gas | 10 [9-10] | 8 [6-9] | 0.0003 | 9 [8-10] | 8 [5-10] | 0.0311 | 0 [0-1] | 1 [0-3] | 0.0056 | 0 [0-1] | 1 [0-5] | 0.1414 |
| 16. Muscle/join pain | 9 [8-10] | 9 [6-10] | 0.0728 | 9 [8-10] | 7.5 [5-10] | 0.1796 | 0 [0-1] | 1 [0-3] | 0.0954 | 0 [0-1] | 2 [0-5.5] | 0.0322 |
| 17. Sex problem | 9 [8-10] | 8 [7-10] | 0.0532 | 9 [8-10] | 8 [5.3-10] | 0.3161 | 0 [0-1] | 0.5 [0-3] | 0.0875 | 0 [0-1] | 0.5 [0-4.5] | 0.3073 |
| 18. Body image | 9 [8.5-10] | 8 [7-10] | 0.0194 | 9 [8-10] | 8 [5.5-9] | 0.0473 | 0 [0-1] | 1 [0-2] | 0.0607 | 0 [0-1] | 1.5 [0-5] | 0.0543 |
| 19. Weight loss | 9 [8-10] | 8 [7-10] | 0.1958 | 9 [8-10] | 7.5 [6-9] | 0.2281 | 0 [0-1] | 1 [0-3] | 0.0791 | 0 [0-1] | 3.5 [1-6.5] | 0.0397 |
| 20. Hair loss | 9 [8-10] | 8 [7-10] | 0.1546 | 9 [8-10] | 10 [7-10] | 0.5411 | 0 [0-1] | 1 [0-2] | 0.1123 | 0 [0-2] | 0 [0-1] | 0.6986 |
| Total | 10 [9-10] | 9 [7-10] | 0.0079 | 9 [9-10] | 8 [6.5-10] | 0.0117 | 0 [0-0] | 0 [0-2] | 0.0207 | 0 [0-1] | 1 [0-3] | 0.0054 |
*Results as Median [Interquartile Range =p25-p75]. HIV Symptoms Index; VAS: visual analogue scale.
Finally, the analysis of the association between the HSI and the VAS demonstrated that at a higher HSI score, the lower level of tolerance according to the VAS (R = –0.51; p < 0.0001), and the higher number of days affected by symptoms according to the VAS (R = 0.51; p < 0.0001).
The total score of the MOS-HIV quality of life questionnaire was 45.71 (SD 2.37) in the physical component among the group of patients with lack of symptoms vs. 42.01 (SD 5.97) among those patients who reported some symptom, with a significant difference (p = 0.04). In terms of the mental component, it was 57.08 (SD 4.14) for lack of symptoms and 51.23 (SD 9.21) in presence of symptoms, also significant (p = 0.02); this confirmed that quality of life was significantly lower in patients with presence of symptoms, even more when only bothersome symptoms were considered.
The MOS-HIV questionnaire score was associated with the HSI score (r = 0.74; p < 0.0001) in the physical health and in the mental health scales (r = 0.67; p < 0.0001); it was significant in both cases. The higher the number of symptoms reported, the lower the quality of life in the physical and mental components in all questionnaire areas, with a correlation rate ranging between 0.34 and 0.74.
The presence of symptoms in the HSI was significantly associated with a worse result both in the physical and the mental components of the MOS- HIV, as appears in Table 4.
Association between the physical and mental components of MOS-HIV and specific symptoms
| MOS-HIV physical health score | MOS-HIV mental health score | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Symptom | Symptom discomfort | Symptom | Symptom discomfort | |||||||||
| Lack | Presence | p-value | Lack | Presence | p-value | Lack | Presence | p-value | Lack | Presence | p-value | |
| 1. Fatigue | 58.7 (5.1) | 50.5 (9.7) | < 0.0001 | 56.8 (6.8) | 43.0 (10.9) | 0.0018 | 55.7 (5.3) | 46.9 (10.3) | < 0.0001 | 53.8 (7.4) | 37.7 (7.2) | 0.0003 |
| 2. Fever | 57.4 (7.5) | 46.4 (10.4) | 0.0006 | 56.5 (6.9) | 36.3 (10.2) | 0.0083 | 53.5 (7.5) | 46.9 (12.1) | 0.0548 | 53.1 (7.9) | 37.2 (10.4) | 0.0174 |
| 3. Dizziness | 58.0 (5.6) | 48.2 (10.2) | 0.0003 | 55.9 (7.9) | 38.4 (−) | 0.1376 | 54.6 (6.2) | 45.7 (11.4) | 0.0030 | 52.5 (8.7) | 49.2 (−) | 0.4284 |
| 4. Hand/foot Pain | 57.6 (5.9) | 49.8 (10.7) | 0.0076 | 57.1 (6.1) | 36.6 (8.3) | 0.0014 | 54.0 (7.0) | 48.0 (11.4) | 0.0331 | 53.5 (7.6) | 38.9 (11.0) | 0.0073 |
| 5. Memory Loss | 58.6 (4.8) | 49.7 (10.1) | 0.0002 | 56.7 (7.0) | 47.3 (11.8) | 0.0168 | 55.9 (6.7) | 45.4 (7.8) | < 0.0001 | 53.5 (8.1) | 44.4 (8.7) | 0.0034 |
| 6. Nausea | 57.5 (6.0) | 51.1 (11.0) | 0.0367 | 56.6 (7.0) | 44.7 (13.9) | 0.0240 | 54.2 (7.1) | 48.0 (10.8) | 0.0418 | 53.6 (7.4) | 37.8 (11.2) | 0.0049 |
| 7. Diarrhea | 56.9 (7.1) | 53.4 (9.4) | 0.1225 | 56.5 (7.0) | 43.9 (13.0) | 0.0093 | 54.0 (7.5) | 49.6 (9.9) | 0.0407 | 53.3 (7.8) | 41.3 (11.9) | 0.0166 |
| 8. Sadness | 58.0 (5.9) | 50.9 (10.1) | 0.0014 | 57.1 (6.0) | 36.2 (7.9) | 0.0003 | 55.9 (6.1) | 45.5 (9.1) | < 0.0001 | 53.9 (7.0) | 33.3 (4.3) | 0.0003 |
| 9. Anxiety | 59.2 (3.9) | 50.9 (9.8) | < 0.0001 | 57.5 (5.5) | 46.8 (12.5) | 0.0065 | 56.5 (5.1) | 47.1 (9.5) | < 0.0001 | 54.2 (7.1) | 44.2 (10.8) | 0.0027 |
| 10. Sleep Trouble | 57.5 (6.3) | 52.5 (9.8) | 0.0242 | 56.9 (6.5) | 48.6 (12.1) | 0.0332 | 55.3 (6.7) | 47.5 (9.3) | 0.0003 | 53.9 (7.7) | 44.9 (9.7) | 0.0033 |
| 11. Skin problems | 57.0 (6.2) | 52.1 (11.0) | 0.1142 | 56.6 (6.8) | 45.6 (13.9) | 0.0269 | 53.8 (7.5) | 49.2 (10.5) | 0.0697 | 53.0 (7.8) | 46.1 (14.2) | 0.1694 |
| 12. Cough | 57.2 (6.2) | 47.9 (11.8) | 0.0066 | 56.3 (6.9) | 30.0 (6.8) | 0.0174 | 53.6 (7.5) | 46.5 (11.4) | 0.0388 | 53.0 (8.0) | 31.5 (1.7) | 0.0231 |
| 13. Headache | 57.2 (6.9) | 51.4 (9.7) | 0.0055 | 56.6 (6.9) | 43.4 (13.6) | 0.0188 | 54.4 (7.7) | 47.3 (8.9) | 0.0006 | 53.2 (8.2) | 43.1 (9.7) | 0.0188 |
| 14. Loss of appetite | 57.0 (6.1) | 51.3 (11.7) | 0.1624 | 56.4 (7.1) | 38.6 (13.5) | 0.0188 | 53.8 (7.6) | 48.3 (10.5) | 0.0455 | 52.9 (8.3) | 41.8 (10.1) | 0.0395 |
| 15. Stomach swelling, pain or gas | 57.9 (5.4) | 52.4 (10.1) | 0.0465 | 57.3 (6.2) | 48.9 (11.3) | 0.0054 | 54.8 (7.0) | 49.2 (9.7) | 0.0081 | 54.1 (7.5) | 45.7 (9.7) | 0.0009 |
| 16. Muscle/join pain | 58.3 (5.7) | 49.9 (9.8) | 0.0001 | 57.5 (6.1) | 43.5 (10.2) | < 0.0001 | 54.4 (7.2) | 48.4 (10.2) | 0.0067 | 54.2 (7.4) | 40.8 (7.8) | < 0.0001 |
| 17. Sex problem | 57.4 (5.5) | 52.3 (11.0) | 0.2681 | 56.9 (6.4) | 46.1 (13.4) | 0.0432 | 54.9 (7.1) | 47.6 (9.3) | 0.0012 | 53.3 (8.2) | 45.7 (9.6) | 0.0287 |
| 18. Body image | 57.6 (6.5) | 52.2 (9.6) | 0.0274 | 57.0 (6.9) | 46.5 (10.2) | 0.0007 | 54.4 (7.5) | 48.9 (9.5) | 0.0152 | 53.7 (8.1) | 44.1 (7.5) | 0.0009 |
| 19. Weight loss | 57.6 (5.7) | 48.9 (11.3) | 0.0039 | 56.2 (7.3) | 46.4 (15.4) | 0.0831 | 54.1 (7.4) | 46.9 (10.2) | 0.0130 | 52.9 (8.4) | 45.4 (10.6) | 0.0831 |
| 20. Hair loss | 56.6 (7.8) | 52.1 (8.6) | 0.0379 | 55.9 (8.1) | 52.0 (8.6) | 0.1574 | 53.4 (8.5) | 48.9 (8.2) | 0.0175 | 52.6 (8.7) | 50.3 (8.4) | 0.2737 |
| Total | 45.71 (2.37) | 42.01 (5.97) | 0.0401 | 44.84 (3.65) | 40.19 (6.47) | 0.0017 | 57.08 (4.14) | 51.23 (9.21) | 0.0211 | 56.34 (6.05) | 47.40 (9.26) | < 0.0001 |
*Results as mean (standard deviation).
The mean adherence, or MPR, during the period before applying the questionnaire (median interval for calculating adherence: 180 days, IQR 150-243) was 94.4% (CI95%: 92.7-96.2), measured through Pharmacy Dispensing Records.
According to the SMAQ Questionnaire, 40% of patients were classified as non-adherent (30/75). Regarding the semi-quantitative Question 5 (doses missed in the past week), 92% of patients considered they had good adherence.
DiscussionThe HSI questionnaire prepared by Justice et al. is the only questionnaire that has been validated for determining and follow-up of symptoms reported by patients on ART, and that is why it was chosen for this pilot trial and subsequent validation in the Spanish population14.
In our study, it was observed that the questionnaire was easy and fast to apply, taking approximately five minutes for each patient to complete. However, there were patients who missed some important matter or symptom, so it was necessary to add the question for other symptoms so that the patient could answer in their own words, though they could be afterwards reclassified among those already existing, or be used to make more detailed questions.
Besides, it presented a good association with the physical and mental dimensions of the MOS-HIV scale, as well as with the level of tolerance according to the VAS. Including a question for Other Symptoms was confirmed as useful, so that the patient could report any symptom not shown in the questionnaire.
The median number of symptoms reported by patients in our pilot study was lower than that stated in the original study by Justice: 5 (IQR 1-10) vs.
15 (IQR 8-19), probably due to the time difference where treatments were worse tolerated. The most frequent symptoms in the study by Justice were fatigue (81%), diarrhea (78%), sadness (76%), sleep disorders (75%) and anxiety (74%), and not very different from those reported by our patients, though again to a lower rate. The study by Justice also showed a good association with the physical and mental dimensions of the MOS-HIV scale, the same as in our study.
In other more recent studies using the same questionnaire, the number of symptoms is 8.2, more similar to our study, and the symptoms most frequently reported by patients are fatigue, sadness, anxiety, insomnia, myalgia, and changes in their physical appearance15–17.
In the study by Braithwaite, 66% of the 1,864 patients in the VACS Veteran Cohort perceived adverse effects associated with ART, though 39% of them had doubts about their real link with the medication18. Among our patients, 81.3% reported some symptom, though only 57% of these were identified as bothersome.
There are other scales, such as the Memorial Symptom Assessment Scale-Short Form (MSAS-SF) which measures the frequency, severity and discomfort associated with 32 symptoms; it has been used in different conditions, particularly for cancer19. In a study by Wakeham K et al., the MSAS-SF was applied to 212 HIV patients with a mean of 14 symptoms: the most frequent symptoms were pain, weight loss, pruritus, tiredness, numbness, coughing, changes in their skin, concern and lack of appetite20. These symptoms agree with those collected among the patients in our pilot study. However, MSAS-SF is a longer and more detailed questionnaire, and with lower experience in HIV.
One of the most important limitations in this study concerns the confusion existing between the symptoms of the disease and those caused by the medications. The HSI questionnaire collects the signs and symptoms reported by the patient, but this does not necessarily mean that these are caused by their antiretroviral medication. Besides, these symptoms can also be affected by the disease or any associated comorbidity presented by the patient.
Another limitation of the study, similar to what happens with any other pilot study, is that we cannot reach final conclusions about the psychometric properties of the questionnaire evaluated. That is why we must wait for the fieldwork results in order to determine the validity and reliability of this instrument.
Regarding mean adherence, differences were observed between the calculation through MPR and the SMAQ; however, when taking into account the semi-quantitative Question 5 in the SMAQ (doses missed during the past week), results were more similar to MPR.
Finally, the results obtained are linked to the type of treatment evaluated in this population; currently, there is a higher use of integrase inhibitors and dual therapy21; therefore, once the questionnaire has been adequately validated, any future lines of research should be oriented to its application in current treatments.
This is an easy to apply and fast questionnaire, well evaluated and with a good level of comprehension by patients; and besides, it presented consistent and significant correlation with the physical and mental dimensions of the MOS-HIV scale, as well as with the tolerance VAS.
The results of our study suggest that the higher the HSI symptom score, the lower tolerance in VAS, a higher frequency of days with poor tolerance according to VAS, and a worse MOS-HIV score in all its dimensions. However, given that this is a pilot study, we consider it necessary to wait for the results of the final study.
FundingNo funding.
AcknowledgementsTo Nerea González Hernández, from the Research Unit of the Hospital de Galdakao, for her support in terms of questionnaire design, development and validation.
Presentation at CongressesResults were presented partially at the 59th Congress of the SEFH, held in Valladolid from September, 30th to October, 3rd, 2014.
Ibarra Barrueta O, Mora Atorrasagasti O, Illaro Uranga A, Morillo Verdugo R, Martín Conde M, Serrano López-De-Las-Hazas J. Estudio piloto para el desarrollo de una herramienta de valoración de la tolerancia al tratamiento antirretroviral. (Pilot study for developing an assessment tool for the tolerance of antiretroviral treatment.) 59th Congress of the SEFH. Valladolid, September, 30th-October, 3rd, 2014.
Conflict of interestsNo conflict of interests.
Contribution to scientific literature
Due to the lack of questionnaires validated for the Spanish population in order to measure the symptoms perceived by the patient with HIV infection, it is suggested to develop and validate a questionnaire based on the HIV Symptoms Index.
Its application in everyday clinical practice can be useful in order to improve the detection and management of treatment-related adverse effects.

