


Comorbidities associated with the ageing of the HIV+ population may require chronic treatment. Our aim is to determine the degree of polypharmacy and the number of potential drug-drug interactions, as well as the relationship between both variables in a HIV-infected population over the age of 65.
MethodsDescriptive transversal study targeting HIV+ patients aged >65, attended in a Spanish hospital in 2014. The prevalence of polypharmacy (>5 drugs) and potential drug-drug interactions were assessed, and also risk factors associated with such.
Results265 subjects aged >65 years were identified, 197 of whom were on antiretroviral treatment and had data about their electronic prescription. 93% were polymedicated. The patients whose antiretroviral treatment included a non-nucleoside reverse transcriptase inhibitor (NNRTI) demonstrated a fourfold probability of being polymedicated. 65% of the patients showed at least one potential drug-drug interaction and 6.6% a severe potential drug-drug interaction. The risk of interaction was significantly associated with the number of prescribed drugs (incidence rate ratio per prescribed drug, CI 95%: 1.18 (1.14;1.22; p<0.0001) and with the use of protease inhibitors (PI) (incidence rate ratio, CI 95%: 1.65 (1.28;2.11; p=0.0001)).
ConclusionPolypharmacy has a high prevalence and is more common in patients treated with NNRTI. The number of potential drug-drug interactions increase with the number of prescribed drugs and is higher in those patients on PI.
Las comorbilidades asociadas al envejecimiento de la población VIH+ pueden requerir tratamientos crónicos. Nuestro objetivo es determinar el grado de polifarmacia y el número de interacciones farmacológicas potenciales, así como la relación entre ambas variables en un grupo de población VIH+ mayor de 65 años.
MétodosEstudio descriptivo transversal en pacientes VIH+>65 años atendidos en un hospital español en 2014. Se evaluó la prevalencia de polimedicación (>5 fármacos) y se analizaron las interacciones farmacológicas potenciales y los factores de riesgo asociados a ellas.
ResultadosSe identificaron 265 sujetos >65 años, de los cuales 197 recibían tratamiento antirretroviral y tenían datos en la receta electrónica. El 93% estaban polimedicados. Los pacientes cuyo tratamiento antirretro- viral incluía un inhibidor de la transcriptasa inversa no nucleósido (ITINN) presentaban una probabilidad cuatro veces mayor de estar polimedica- dos. El 65% de los pacientes presentó al menos una interacción potencial y el 6,6% una interacción potencial grave. El riesgo de interacciones se asoció significativamente al número de fármacos prescritos (razón de tasas de incidencia por fármaco prescrito con IC 95%: 1,18 (1,14;1,22; p<0.0001)) y a los inhibidores de la proteasa (IP) (razón de tasas de incidencia IC 95%: 1,65 (1,28;2,11; p=0,0001)).
ConclusiónLa prevalencia de la polifarmacia es muy alta y más frecuente en los pacientes tratados con ITINN. El número de interacciones farmacológicas potenciales aumenta con el número de fármacos prescritos y es mayor en los pacientes tratados con IP.
Although it is currently not possible to eradicate HIV infection, high activity antiretroviral therapy (ART) has made it possible to reduce mortality and turn it into a chronic disease.
Life expectancy for the general population in Spain is increasingly longer, being in 2014 of 85.6 years for women and 80.1 years for men. There is a progressively growing number of people over the age of 65 and a parallel increase in comorbidity that require chronic treatment. The same is true for the population infected by HIV1.
Polypharmacy or polymedication is associated with greater complexity in the management of therapeutic treatment and with increased risk of adverse events and drug-drug interactions, mismedication, reduced adherence to treatment and falls2. It is also related to an increase in hospitalisation and mortality3. Taking into account that standard ART is based on the simultaneous administration of 3 different drugs4, polypharmacy is common1. Nevertheless, there is little data on the population infected by HIV over the age of 65.
Therefore, the aim of this study is to determine the level of polypharmacy and the number of potential drug-drug interactions, as well as the relationship between both variables, in a group of patients infected by HIV over the age of 65 belonging to a large cohort of HIV+ patients.
MethodsDescriptive cross-sectional study conducted at a tertiary Spanish university hospital with over 4,500 HIV-infected patients under active followup. It included all patients >65 years of age who received antiretroviral treatment and had a chronic medication record in the CatSalut's Electronic Prescription System (SIRE) in November 2014. Transfers and exitus were excluded. Polypharmacy was defined as taking 5 or more drugs2. Clinical variables (time since HIV diagnosis, HIV transmission mode, acquired immune deficiency syndrome (AIDS) diagnosis, viral load, CD4 lymphocyte count and hepatitis C virus serology) and demographics (age and gender) were evaluated, as well as the ART and concomitant medication, which was classified according to the Anatomical Therapeutic Chemical (ATC) Classification System.
A screening for potential drug-drug interactions was conducted with the HIV Interactions database from the Hospital Clinic de Barcelona5 and the HIV Drug Interactions database from the University of Liverpool6. Later, they were classified according to their relevance, defining them as moderate if they required monitoring/dosage adjustment and severe if their concomitant use was contraindicated/not recommended5,6. They were also classified according to whether the interaction type was pharmacokinetic or pharmacodynamic, and whether it affected the ART or the chronic medication.
The study was not assessed by a clinical research ethics board, as it was not deemed to affect the care given to the patients at the hospital.
The statistical analysis was conducted with version 13 of the Stata program. The categorical variables were expressed with absolute frequencies and percentages. The continuous variables with average and standard deviation (SD) or median and interquartile range (IQR). To evaluate possible differences between the polymedicated and non-polymedicated groups of patients, the Chi-squared test or the Fisher's exact test was used for qualitative variables and the Student's t-testor Mann-Whitney U test for quantitative variables. A logistical regression was conducted to identify factors (demographic, clinical and ART) associated with polymedication and a Poisson regression to assess variables associated with the incidence of interactions. Bilateral values of p<0.05 were considered statistically significant.
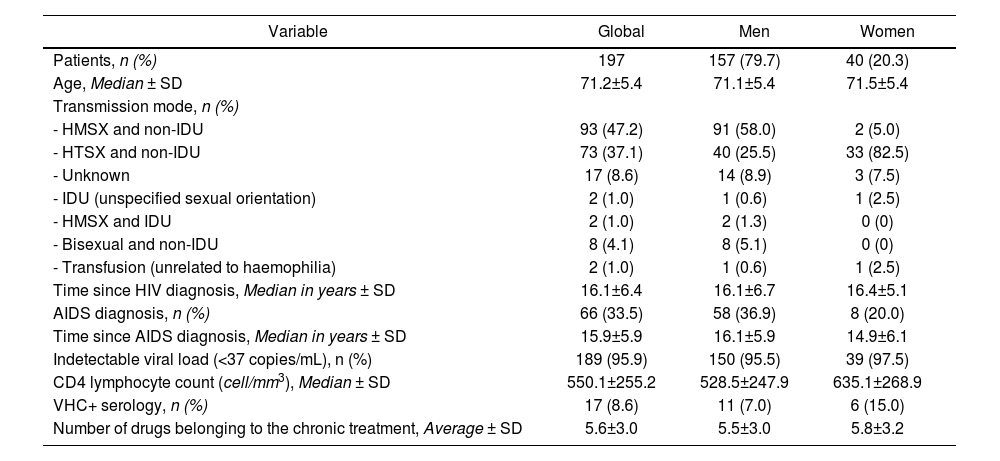
ResultsIn our cohort of HIV+ patients, we identified 6% (n=265) of subjects >65 years. Sixty-eight patients were excluded due to transfer to other regions (n=2), exitus (n=7), lack of data in SIRE (n=58) or because of not receiving antiretroviral therapy (n=1). The remaining 197 patients were included in the study. 80% were men and the average age was 71 years. The characteristics of the population are summarised in table 1. The statistical analysis showed no significant differences in the demographic and clinical variables between polymedicated and non-polymedicated patients.
Characteristics of the HIV-positive population ≥ 65 years
| Variable | Global | Men | Women |
|---|---|---|---|
| Patients, n (%) | 197 | 157 (79.7) | 40 (20.3) |
| Age, Median ± SD | 71.2±5.4 | 71.1±5.4 | 71.5±5.4 |
| Transmission mode, n (%) | |||
| - HMSX and non-IDU | 93 (47.2) | 91 (58.0) | 2 (5.0) |
| - HTSX and non-IDU | 73 (37.1) | 40 (25.5) | 33 (82.5) |
| - Unknown | 17 (8.6) | 14 (8.9) | 3 (7.5) |
| - IDU (unspecified sexual orientation) | 2 (1.0) | 1 (0.6) | 1 (2.5) |
| - HMSX and IDU | 2 (1.0) | 2 (1.3) | 0 (0) |
| - Bisexual and non-IDU | 8 (4.1) | 8 (5.1) | 0 (0) |
| - Transfusion (unrelated to haemophilia) | 2 (1.0) | 1 (0.6) | 1 (2.5) |
| Time since HIV diagnosis, Median in years ± SD | 16.1±6.4 | 16.1±6.7 | 16.4±5.1 |
| AIDS diagnosis, n (%) | 66 (33.5) | 58 (36.9) | 8 (20.0) |
| Time since AIDS diagnosis, Median in years ± SD | 15.9±5.9 | 16.1±5.9 | 14.9±6.1 |
| Indetectable viral load (<37 copies/mL), n (%) | 189 (95.9) | 150 (95.5) | 39 (97.5) |
| CD4 lymphocyte count (cell/mm3), Median ± SD | 550.1±255.2 | 528.5±247.9 | 635.1±268.9 |
| VHC+ serology, n (%) | 17 (8.6) | 11 (7.0) | 6 (15.0) |
| Number of drugs belonging to the chronic treatment, Average ± SD | 5.6±3.0 | 5.5±3.0 | 5.8±3.2 |
AIDS: Acquired Immune Deficiency Syndrome; HCV: Hepatitis C Virus; HIV: Human Immunodeficiency Virus; HMSX: Homosexual; HTSX: Heterosexual; IDU: Intravenous Drug User; SD: standard deviation.
One hundred and eighty-three patients (93%) were polymedicated. The average ± SD of drugs associated with the ART was 5.6 ± 3.0 and most of them were used to treat diseases associated with the cardiovascular system, metabolism and the central nervous system.
57% of the patients received 2 nucleoside reverse-transcriptase inhibitors (NRTI) and 1 non-nucleoside reverse-transcriptase inhibitors (NNRTI), 33% 2 NRTI and 1 protease inhibitors (PI), 20% 2 NRTI with one integrase inhibitor (INI). A single patient could receive drugs from several of these families. The remaining 1% used other less common combinations. In the logistical regression model, patients whose ART included a NNRTI had a significantly higher probability of being polymedicated (OR adjusted for age with CI 95%: 4.29 (1.27;14.52); p=0.0193).
65% of the patients had at least one potential drug-drug interaction, and 6.6% had a severe potential interaction. 33% had two or more potential interactions. A total of 259 potential interactions were detected, of which 92% were pharmacokinetic and the rest (8%) pharmacodynamic. 82% of the interactions affected only the drug belonging to the chronic medication, 8% affected only the ART and 10% affected both. Of the interactions that affected the drug from the chronic medication, 56% compromised the efficacy of the treatment, while 42% could cause toxicity. The consequence of the interaction is unknown in 4 cases, although they probably could have affected efficacy or toxicity. Amongst the interactions that affected the ART, 45% could reduce efficacy and 55% could increase toxicity.
Interactions were observed in 72% of the patients treated with PIs, in 68% of the patients with NNRTIs and in 51% of those treated with INIs. The number of interactions was significantly higher in patients treated with PIs compared to the rest (incidence rate ratio with CI 95%: 1.65 (1.28;2.11); p=0.0001).
Also, a statistically significant association was observed between the number of prescribed drugs and the number of interactions (incidence rate ratio by prescribed drug with CI 95%: 1.18 (1.14;1.22); p<0.0001).
Figure 1 shows the prevalence of potential drug-drug interactions based on the number of prescribed drugs and antiretroviral treatment.
![Prevalence of potential drug-drug interactions based on the number of prescribed drugs and antiretroviral treatment. Based on the type of antiretroviral treatment, you can see, on the x-axis, the total number of drugs (including antiretroviral treatment [combination of 3 drugs] and the treatment belonging to chronic medication) and, on the y-axis: the total number of patients receiving it, number of patients with at least a moderate potential drug-drug interaction and number of patients with a severe potential drug-drug interaction.](https://static.elsevier.es/multimedia/11306343/0000004100000005/v1_202311080532/S1130634323004804/v1_202311080532/en/main.assets/gr1.jpeg?xkr=ue/ImdikoIMrsJoerZ+w9+opCvKj0krr07z/sBozKi4kBXacr+lRMWrGb15lwQutRYwcrgjtjjx1uM7ZKbixJWIw/1BfObKj3DuH1HogiatlZKgfZQozn5r3zR1ZZu2VqXgexp4meCNiwGwwVDnTLBKGpuNHvUvgNJTGMCztIKz5BSD/O5pp9MB2aT7SH9AeNzvsBPTea3sNhfNKN+dbBALEb0DUklk1rT1+Nt9R++vFTotnayALuuPPueR2UoPRSY6dZFJVat9RJhWN3fPaZc56A4EJdGN6xK/8diUAI/0= "Prevalence of potential drug-drug interactions based on the number of prescribed drugs and antiretroviral treatment. Based on the type of antiretroviral treatment, you can see, on the x-axis, the total number of drugs (including antiretroviral treatment [combination of 3 drugs] and the treatment belonging to chronic medication) and, on the y-axis: the total number of patients receiving it, number of patients with at least a moderate potential drug-drug interaction and number of patients with a severe potential drug-drug interaction.")
Prevalence of potential drug-drug interactions based on the number of prescribed drugs and antiretroviral treatment. Based on the type of antiretroviral treatment, you can see, on the x-axis, the total number of drugs (including antiretroviral treatment [combination of 3 drugs] and the treatment belonging to chronic medication) and, on the y-axis: the total number of patients receiving it, number of patients with at least a moderate potential drug-drug interaction and number of patients with a severe potential drug-drug interaction.
Regarding associated chronic treatment, the risk of interaction was significantly higher in patients that received drugs to treat pathologies of the alimentary tract and metabolism (ATC: group A; incidence rate ratio with CI 95%: 1.99 (1.44;2.75, p<0.0001)), nervous system (ATC: group N; incidence rate ratio with CI 95%: 1.72 (1.32;2.23, p<0.0001)), genito urinary system and sex hormones (ATC: group G; incidence rate ratio with CI 95%: 1.67 (1.28;2.18, p<0.0001)), musculo-skeletal system (ATC: group M; incidence rate ratio with CI 95%: 1.61 (1.20;2.15, p<0.0015)), cardiovascular system (ATC: group C; incidence rate ratio with CI 95%: 1.57 (1.12;2.21, p=0.0083)) and of the blood and blood forming organs (ATC: group B; incidence rate ratio with CI 95%: 1.29 (1.01;1.65, p=0.0413)).
DiscussionThe results of our study confirm that polymedication is almost universal in patients over the age of 65. Marzolini et al. agree that polypharmacy is common in the population of elderly HIV-infected adults1. The prevalence of polymedication in our cohort (93%) is greater than described by Guthrie et al. in the general population in Scotland7. These authors found that, in 2010, approximately 40% of patients over the age of 65 took > 5 drugs and 10% >10 drugs. This major difference in prevalence of polymedication may possibly be due to the fact that the appearance of comorbidities associated with age occurs 10 years sooner in the HIV+ population than in the general population and that ART itself includes 3 drugs8. As a consequence, there is an earlier use of medication for the treatment of these comorbidities in the HIV-positive population. The types of drugs most commonly used in our cohort of patients coincides with previous studies1,2,9, with a greater use of statins, antihypertensives, antacids, vitamins, antidiabetics, antidepressant, antipsychotics and androgens.
As regards the demographic characteristics, as in previous studies1,2, in our study's population there was a predominance of male patients and the primary mode of HIV transmission was men who had sex with men. In this age group, no differences were observed compared to the rest of our cohort.
Approximately two-thirds of our patients had some potential drug-drug interaction, and 6.6% had a severe potential interaction. Most were pharmacokinetic and were related to non-antiretroviral drugs, as in the studies of Marzolini et al.1 and Greene et al.2.
The results show that the probability of drug-drug interaction increases with the number of prescribed drugs, illustrating one of the consequences of polypharmacy. Besides, the greater prevalence of interactions in patients treated with PIs suggests that the use of INIs or NNRTIs would be a safer option in polymedicated patients. Thus, the differences in the ART used in the polymedicated and non-polymedicated groups (lower use of PIs and greater use of NNRTIs in polymedicated patients) can be explained, in part, by the intent to avoid drug-drug interactions.
Our results, similar to those observed in other studies8,10, indicate that special attention should be paid in patients treated with PIs. A high risk of interactions is also estimated in patients treated with cobicistat, although at the time of the study, only two patients received it, as it was just starting to be used as part of the ART. Nor should we forget the interactions between chronic non-antiretroviral medication drugs, which have not been assessed in our study.
One limitation of the study is that we are not aware of the current situation of the 58 patients with no data in the SIRE; that is, we do not actually know whether they did not receive other drugs or their treatmentwas not recorded. However, we must highlight that the study was conducted in one of the largest cohorts of patients infected with HIV in our country.
In conclusion, our results provide evidence that the prevalence of polypharmacy in elderly HIV+ patients is very high and more frequent in patients treated with NNRTIs. The number of potential drug-drug interactions increases with the number of prescribed drugs and is greater in patients treated with PIs. These data support the need to change the care given to patients with HIV2, periodically reviewing the medication and incorporating the guidelines for drug usage in the elderly, which should be adapted to the population infected with HIV10. Given its complexity, a multidisciplinary approach is required.
Our study was conducted in one of the largest cohorts of patients infected by HIV in our country. In particular, it analyses a group of patients that will be increasingly relevant in clinical practice because advances in the pharmacological approach for the management of the disease have enabled the HIV-positive population to age.
Our results provide information on the prevalence of polypharmacy in said subjects, illustrating that it is a nearly universal situation in patients over the age of 65. Potential drug-drug interactions derived from polypharmacy were also analyzed, contributing data on its prevalence and clinical relevance.
Finally, we identify the drug groups belonging to chronic medication with a high risk of drug-drug interaction, as well as the antiretroviral classes with high risk.
There is little data on elderly patients infected by HIV over 65 years, so our results may be of interest in clinical practice. We bring to light the need to change the care given to HIV patients, which should focus on a multidiscipline approach due to its high complexity. Periodic reviews of the medication should be promoted, as well as the inclusion of drug usage guidelines for the elderly adapted to the HIV-positive population.
La erradicación de la infección por VIH no es posible en la actualidad, aunque el tratamiento antirretroviral (TAR) de gran actividad ha permitido reducir la mortalidad y convertirla en una enfermedad crónica.
La esperanza de vida de la población general en España es cada vez mayor, siendo en 2014 de 85,6 años en mujeres y de 80,1 años en hombres. El número de personas mayores de 65 años es progresivamente mayor y también el aumento paralelo de comorbilidades que precisan tratamiento crónico. Lo mismo sucede en la población con infección por el VIH1.
La polifarmacia o polimedicación se asocia a una mayor complejidad del manejo terapéutico e incrementa el riesgo de efectos adversos e interacciones, errores de medicación, reducción de la adherencia al tratamiento y caídas2. También se ha relacionado con un aumento de hospitalizaciones y de morta- lidad3. Teniendo en cuenta que el TAR estándar se basa en la administración simultánea de 3 fármacos distintos4, la polifarmacia es frecuente1, aunque existen pocos datos en población con infección por el VIH mayor de 65 años.
Los objetivos de este estudio son determinar el grado de polifarmacia y el número de interacciones farmacológicas potenciales, así como la relación entre ambas variables, en un grupo de pacientes con infección por el VIH mayores de 65 años pertenecientes a una gran cohorte de pacientes VIH+.
MétodosEstudio descriptivo transversal realizado en un hospital universitario español de tercer nivel con más de 4.500 pacientes con infección por el VIH en seguimiento activo. Se incluyeron todos los pacientes >65 años que recibieran tratamiento antirretroviral y tuvieran registro de medicación crónica en el Sistema Integral de Receta Electrónica (SIRE) del CatSalut en noviembre de 2014. Se excluyeron trasladados y exitus. Se definió polifarmacia como la toma de 5 o más fármacos2. Se evaluaron variables clínicas (tiempo desde diagnóstico del VIH, vía de transmisión del VIH, diagnóstico de síndrome de inmunodefi- ciencia adquirida (SIDA), carga viral, recuento de linfocitos CD4 y serología virus hepatitis C) y demográficas (edad y sexo), así como el TAR y medicación concomitante, que se clasificó según el Sistema de Clasificación Anatómica, Terapéutica, Química (ATC).
Se realizó un cribado de interacciones farmacológicas potenciales mediante las bases de datos Interacciones VIH del Hospital Clínic de Barcelona5 y HIV Drug Interactions de la Universidad de Liverpool6. Posteriormente, se clasificaron según su relevancia, definiéndose como moderadas si requerían monitorización/ajuste de dosis y como graves si su uso concomitante estaba contraindicado/no recomendado5,6. También se clasificaron según si el tipo de interacción era farmacocinética o farmacodinámica, y si afectaba al TAR o a la medicación crónica.
El estudio no fue evaluado por un comité de ética de investigación clínica al considerarse que su desarrollo no cambiaba la atención que los pacientes recibían en el hospital.
El análisis estadístico se llevó a cabo con la versión 13 del programa Stata. Las variables categóricas se expresaron con frecuencias absolutas y porcentajes. Las variables continuas con media y desviación estándar (DE) o mediana y rango intercuartílico (RIQ). Para evaluar si existían diferencias entre el grupo de pacientes polimedicados y no polimedicados se usó la prueba Chi-cuadrado o el test exacto de Fisher para las variables cualitativas y el t-test o U de MannWhitney para las cuantitativas. Se realizó una regresión logística para identificar los factores (demográficos, clínicos y TAR) asociados a la polimedi- cación y una regresión de Poisson para evaluar las variables asociadas a la incidencia de interacciones. Valores de p<0,05 bilaterales se consideraron estadísticamente significativos.
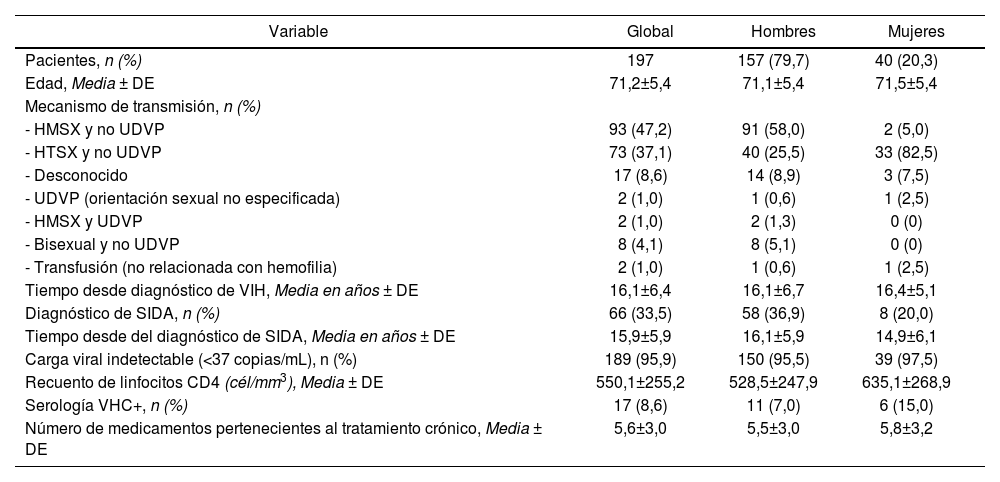
ResultadosDe nuestra cohorte de pacientes VIH+, se identificaron un 6% (n=265) de sujetos >65 años. Sesenta y ocho pacientes fueron excluidos por traslado a otras comunidades autónomas (n=2), exitus (n=7), falta de datos en SIRE (n=58) o por no recibir tratamiento antirretroviral (n=1). Se incluyeron en el estudio los 197 pacientes restantes. El 80% eran hombres y la media de edad de 71 años. Las características de la población se resumen en la tabla 1. El análisis estadístico no mostró diferencias significativas en las variables demográficas y clínicas entre pacientes polimedicados y no polimedicados.
Características de la población VIH positiva ≥ 65 años
| Variable | Global | Hombres | Mujeres |
|---|---|---|---|
| Pacientes, n (%) | 197 | 157 (79,7) | 40 (20,3) |
| Edad, Media ± DE | 71,2±5,4 | 71,1±5,4 | 71,5±5,4 |
| Mecanismo de transmisión, n (%) | |||
| - HMSX y no UDVP | 93 (47,2) | 91 (58,0) | 2 (5,0) |
| - HTSX y no UDVP | 73 (37,1) | 40 (25,5) | 33 (82,5) |
| - Desconocido | 17 (8,6) | 14 (8,9) | 3 (7,5) |
| - UDVP (orientación sexual no especificada) | 2 (1,0) | 1 (0,6) | 1 (2,5) |
| - HMSX y UDVP | 2 (1,0) | 2 (1,3) | 0 (0) |
| - Bisexual y no UDVP | 8 (4,1) | 8 (5,1) | 0 (0) |
| - Transfusión (no relacionada con hemofilia) | 2 (1,0) | 1 (0,6) | 1 (2,5) |
| Tiempo desde diagnóstico de VIH, Media en años ± DE | 16,1±6,4 | 16,1±6,7 | 16,4±5,1 |
| Diagnóstico de SIDA, n (%) | 66 (33,5) | 58 (36,9) | 8 (20,0) |
| Tiempo desde del diagnóstico de SIDA, Media en años ± DE | 15,9±5,9 | 16,1±5,9 | 14,9±6,1 |
| Carga viral indetectable (<37 copias/mL), n (%) | 189 (95,9) | 150 (95,5) | 39 (97,5) |
| Recuento de linfocitos CD4 (cél/mm3), Media ± DE | 550,1±255,2 | 528,5±247,9 | 635,1±268,9 |
| Serología VHC+, n (%) | 17 (8,6) | 11 (7,0) | 6 (15,0) |
| Número de medicamentos pertenecientes al tratamiento crónico, Media ± DE | 5,6±3,0 | 5,5±3,0 | 5,8±3,2 |
DE: desviación estándar; HMSX: Homosexual; HTSX: Heterosexual; SIDA: Síndrome de inmunodeficiencia adquirida; UDVP: Usuario de drogas vía parenteral; VHC: Virus Hepatitis C; VIH: Virus de inmunodeficiencia humana.
Ciento ochenta y tres pacientes (93%) estaban polimedicados. La media ± DE de fármacos asociados al TAR fue de 5,6 ± 3,0 y en su mayoría iban dirigidos a tratar enfermedades asociadas al sistema cardiovascular, metabolismo y sistema nervioso central.
Un 57% de los pacientes recibían 2 inhibidores de la transcriptasa inversa análogos de nucleósidos (ITIAN) y 1 inhibidor de la transcriptasa inversa no nu- cleósido (ITINN), 33% 2 ITIAN y 1 inhibidor de la proteasa (IP), 20% 2 ITIAN con un inhibidor de la integrasa (INI). Un mismo paciente podía recibir fármacos de varias de estas familias. El 1% restante emplearon otras combinaciones menos frecuentes. En el modelo de regresión logística, los pacientes cuyo TAR incluía un ITINN presentaban una probabilidad significativamente mayor de estar polimedicados (OR ajustado por edad con IC95%: 4,29 (1,27;14,52); p=0,0193).
El 65% de pacientes presentaron al menos una interacción farmacológica potencial y el 6,6% una interacción potencial grave. El 33% tuvieron dos o más interacciones potenciales. Se detectó un total de 259 interacciones potenciales, de las cuales el 92% eran farmacocinéticas y el resto (8%) farmacodiná- micas. El 82% de las interacciones afectaron sólo al fármaco perteneciente a la medicación crónica, el 8% afectaron sólo al TAR y el 10% a ambos. De las interacciones que afectaron al fármaco de la medicación crónica, un 56% comprometían la eficacia del tratamiento mientras que el 42% podían causar toxicidad. Se desconoce el sentido de la interacción en 4 de los casos, aunque probablemente pudieran afectar a la eficacia o toxicidad. De las interacciones que afectaron al TAR, el 45% podían reducir su eficacia y el 55% podían aumentar su toxicidad.
Se observaron interacciones en un 72% de los pacientes tratados con IP, en un 68% de los pacientes con ITINN y en un 51% de los tratados con INI. El número de interacciones fue significativamente mayor en aquellos pacientes tratados con IP en comparación con el resto (razón de tasas de incidencia IC 95%: 1,65 (1,28;2,11); p=0,0001).
También se observó una asociación estadísticamente significativa entre el número de fármacos prescritos y el número de interacciones (razón de tasas de incidencia por fármaco prescrito con IC 95%: 1,18 (1,14;1,22); p<0.0001).
La figura 1 muestra la prevalencia de interacciones farmacológicas potenciales en función del número de fármacos prescritos y tratamiento antirretroviral.
![Prevalencia de interacciones farmacológicas potenciales en función del número de fármacos prescritos y tratamiento antirretroviral. En función de la clase de tratamiento antirretroviral, puede observarse en abscisas el número total de medicamentos (incluye el tratamiento antirretroviral [combinación de 3 fármacos] y el tratamiento perteneciente a la medicación crónica) y en ordenadas: el número de pacientes totales que lo reciben, número de pacientes que presentaban una interacción farmacológica potencial como mínimo de carácter moderado y número de pacientes con una interacción farmacológica potencial grave.](https://static.elsevier.es/multimedia/11306343/0000004100000005/v1_202311080532/S1130634323004804/v1_202311080532/en/main.assets/gr1a.jpeg?xkr=ue/ImdikoIMrsJoerZ+w9+opCvKj0krr07z/sBozKi4kBXacr+lRMWrGb15lwQutRYwcrgjtjjx1uM7ZKbixJWIw/1BfObKj3DuH1HogiatlZKgfZQozn5r3zR1ZZu2VqXgexp4meCNiwGwwVDnTLBKGpuNHvUvgNJTGMCztIKz5BSD/O5pp9MB2aT7SH9AeNzvsBPTea3sNhfNKN+dbBALEb0DUklk1rT1+Nt9R++vFTotnayALuuPPueR2UoPRSY6dZFJVat9RJhWN3fPaZc56A4EJdGN6xK/8diUAI/0= "Prevalencia de interacciones farmacológicas potenciales en función del número de fármacos prescritos y tratamiento antirretroviral. En función de la clase de tratamiento antirretroviral, puede observarse en abscisas el número total de medicamentos (incluye el tratamiento antirretroviral [combinación de 3 fármacos] y el tratamiento perteneciente a la medicación crónica) y en ordenadas: el número de pacientes totales que lo reciben, número de pacientes que presentaban una interacción farmacológica potencial como mínimo de carácter moderado y número de pacientes con una interacción farmacológica potencial grave.")
Prevalencia de interacciones farmacológicas potenciales en función del número de fármacos prescritos y tratamiento antirretroviral. En función de la clase de tratamiento antirretroviral, puede observarse en abscisas el número total de medicamentos (incluye el tratamiento antirretroviral [combinación de 3 fármacos] y el tratamiento perteneciente a la medicación crónica) y en ordenadas: el número de pacientes totales que lo reciben, número de pacientes que presentaban una interacción farmacológica potencial como mínimo de carácter moderado y número de pacientes con una interacción farmacológica potencial grave.
Respecto al tratamiento crónico asociado, el riesgo de interacción fue significativamente mayor en los pacientes que recibían fármacos para tratar patologías del tracto alimentario y metabolismo (ATC: grupo A; razón de tasas de incidencia con IC 95%: 1,99 (1,44;2,75, p <0,0001)), sistema nervioso central (ATC: grupo N; razón de tasas de incidencia con IC 95%: 1,72 (1,32;2,23, p <0,0001)), genitourinario (ATC: grupo G; razón de tasas de incidencia con IC 95%: 1,67 (1,28;2,18, p=0,0001)), sistema musculoesquelético (ATC: grupo M; razón de tasas de incidencia con IC 95%: 1,61 (1,20;2,15, p=0,0015)), sistema cardiovascular (ATC: grupo C; razón de tasas de incidencia con IC 95%: 1,57 (1,12;2,21, p=0,0083)) y de la sangre y órganos hematopoyéticos (ATC: grupo B; razón de tasas de incidencia con IC 95%: 1,29 (1,01;1,65, p=0,0413)).
DiscusiónLos resultados de nuestro estudio confirman que la polimedicación es un hecho casi universal en los pacientes mayores de 65 años. Marzolini et al. coinciden en que la polifarmacia es común en la población de adultos mayores infectados por VIH1. La prevalencia de polimedicación en nuestra cohorte (93%) es superior a la descrita por Guthrie et al. en población general en Escocia7. Estos autores hallaron que, en el año 2010, aproximadamente el 40% de los pacientes mayores de 65 años tomaban > 5 fármacos y el 10% >10 fármacos. Posiblemente, esta gran diferencia en prevalencia de polimedicación se deba a que la aparición de comorbilidades asociadas a la edad se produce 10 años antes en población VIH+ que en la población general8. Como consecuencia, existe un uso más precoz de medicación para el tratamiento de dichas comorbilidades en la población seropositiva. Las clases de fármacos más consumidas en nuestra cohorte de pacientes coinciden con estudios previos1,2,9, evidenciándose un mayor uso de estatinas, antihipertensivos, antiácidos, vitaminas, hipoglucemiantes, antidepresivos, antipsicóticos y andrógenos.
En cuanto a las características demográficas, al igual que en estudios previos1,2, en la población de nuestro estudio hubo un predominio del sexo masculino y el principal modo de transmisión del VIH fue hombres que tienen sexo con hombres, no observándose diferencias en este grupo de edad con el resto de nuestra cohorte.
Aproximadamente dos tercios de nuestros pacientes presentaron alguna interacción farmacológica potencial y el 6,6% una interacción potencial grave La mayoría fueron farmacocinéticas e implicaron más a los fármacos no antirretrovirales, como en los estudios de Marzolini et al.1 y Greene et al.2.
Los resultados demuestran que la probabilidad de interacción farmacológica aumenta con el número de fármacos prescritos, poniendo de manifiesto una de las consecuencias de la polifarmacia. La mayor prevalencia de interacciones en los pacientes tratados con IP sugiere que el uso de INI o ITINN sería una alternativa más segura en pacientes polimedicados. Las diferencias en el TAR empleado en los grupos de po- limedicados y no polimedicados (menor uso de IP y mayor uso de ITINN en los polimedicados) pueden explicarse, en parte, por la intención de evitar interacciones farmacológicas.
Nuestros resultados, similares a los observados en otros estudios8,10, indican que debería prestarse especial atención a las interacciones en los pacientes tratados con IP. También se estima un riesgo de interacciones elevado en aquellos pacientes en tratamiento con cobicistat aunque en el momento del estudio, sólo dos pacientes lo recibían ya que justo se empezaba a usar como parte del TAR. Tampoco debemos olvidar las interacciones entre fármacos no antirretrovirales pertenecientes a la medicación crónica, que no han sido evaluadas en nuestro estudio.
Una limitación del estudio es que desconocemos la situación real de los 58 pacientes sin datos en el SIRE; es decir, no sabemos realmente si no recibían otros fármacos o si tomaban otros tratamientos que no estuvieran registrados. Sin embargo, debemos resaltar que el estudio se ha llevado a cabo en una de las cohortes de pacientes con infección por el VIH más extensas de nuestro país.
En conclusión, nuestros resultados proporcionan evidencia de que la prevalencia de la polifarmacia en pacientes mayores VIH+ es muy alta y más frecuente en pacientes tratados con ITINN. El número de interacciones farmacológicas potenciales aumenta con el número de fármacos prescritos y es mayor en pacientes tratados con IP. Estos datos apoyan la necesidad de un cambio en la atención del paciente con VIH2, realizando revisiones periódicas de la medicación e incorporando las guías de uso de fármacos en edad avanzada, que deberán adaptarse a la población con infección por el VIH10. Dada la complejidad, es necesario un abordaje multidisciplinario.
Nuestro estudio se llevó a cabo en una de las cohortes de pacientes con infección por el VIH más extensas de nuestro país. En concreto, analiza un grupo de pacientes que cada vez va a tener más relevancia en la práctica clínica, debido a que los avances en el tratamiento de la enfermedad están permitiendo un envejecimiento de la población VIH positiva.
Nuestros resultados aportan datos sobre la prevalencia de la poli- farmacia en dichos sujetos, poniendo de manifiesto que se trata de una situación casi universal en pacientes mayores de 65 años. También se analizan las interacciones farmacológicas potenciales derivadas de la polifarmacia, aportando datos de su prevalencia y relevancia clínica. Finalmente, identificamos aquellos grupos de fármacos pertenecientes a la medicación crónica con mayor riesgo de presentar una interacción farmacológica, así como las clases de tratamiento antirretroviral con mayor riesgo.
Existen pocos datos en población con infección por el VIH muy envejecida (> 65 años) por lo que nuestros resultados pueden ser de interés en la práctica clínica. Ponemos de manifiesto la necesidad de un cambio en la atención del paciente con VIH, que debería centrarse en un abordaje multidisciplinar debido a su alta complejidad. Se deberían potenciar revisiones periódicas de la medicación y la incorporación de guías de uso de fármacos en edad avanzada adaptadas a la población con infección por el VIH.


Farmacia Hospitalaria sigue las recomendaciones para la preparación, presentación y publicación de trabajos académicos en revistas biomédicas
- Inicio
- Todos los contenidos
- Publique su artículo
- Acerca de la revista
- Métricas